P/CHD

Yue-Hin Loke, MD
Associate Professor
Children's National Medical Center
Yue-Hin Loke, MD
Associate Professor
Children's National Medical Center
Ryan P. O'Hara, PhD
Postdoc
Children's National Hospital
Sarah E. Kollar, DO
Advanced Imaging Cardiologist
Children's National Hospital
Ravi Vamsee Vegulla, MD
Assistant Professor of Pediatrics
Children's National Medical Center
Elias Balaras, PhD
Professor
George Washington University

Tarek Alsaied, MD
Assistant Professor of Pediatrics
Children's Hospital of Pittsburgh
.png "Laura Olivieri, MD photo")
Laura Olivieri, MD
Associate Professor of Pediatrics
Children's Hospital of Pittsburgh of UPMC

Rahul H. Rathod, MD, MBA
Associate Chair of Cardiology
Boston Children's Hospital
.jpg "Uyen Truong, MD photo")
Uyen Truong, MD
Associate Professor
Children's National Hospital
Francesco Capuano, PhD
Assistant Professor
Universitat Politecnica deCatalunya Barcelona Tech, Spain
The systemic right ventricle (RV) in hypoplastic left heart syndrome (HLHS) patients is subject to abnormal loading conditions and dysfunction. Conventional volumetric/strain parameters (ejection fraction/EF, RV end-diastolic volume/RVEDVi and global circumferential strain/GCS) do not describe the interplay between myocardial work and intracardiac blood flow. Hemodynamic force (HDF) analysis provides a novel characterization of the global intraventricular pressure gradients in heart failure patients, derived from the moving boundary of the ventricular endocardium in cine imaging. In this study, we analyzed HDF in a large multi-center cohort of HLHS patients and determined associations with clinical outcomes.
Methods:
Two hundred and eighty-four studies from unique HLHS patients in the Fontan Outcomes Registry using CMR Examinations (FORCE) were post-processed by a core lab at one institution, including volumetry and phase-contrast measurements. Studies with significant cine artifact were excluded. Feature-tracking (QStrain, Medis) captured RV wall motion from long-axis/short-axis cine. 3D end-diastolic models of RV were reconstructed using Mimics (Materialise). A diffeomorphic mapping technique was used to calculate 3D RV kinematic models and derive the global HDF vector throughout the cardiac cycle. HDF was further separated into three directions for analysis: Apical-to-Basal, Septal-to-Free Wall, and Inferior-to-Anterior (Fig 1). HDF parameters were indexed to volume and RR interval (N/L*s2). The root mean square (rms) magnitude of HDF parameters were compared against a cohort of twenty healthy controls with normal RV size/function. Relationships between HDF parameters and composite adverse outcomes (mortality/transplant, transplant listing, plastic bronchitis, protein losing enteropathy) were assessed using bivariable regression analyses.
Results:
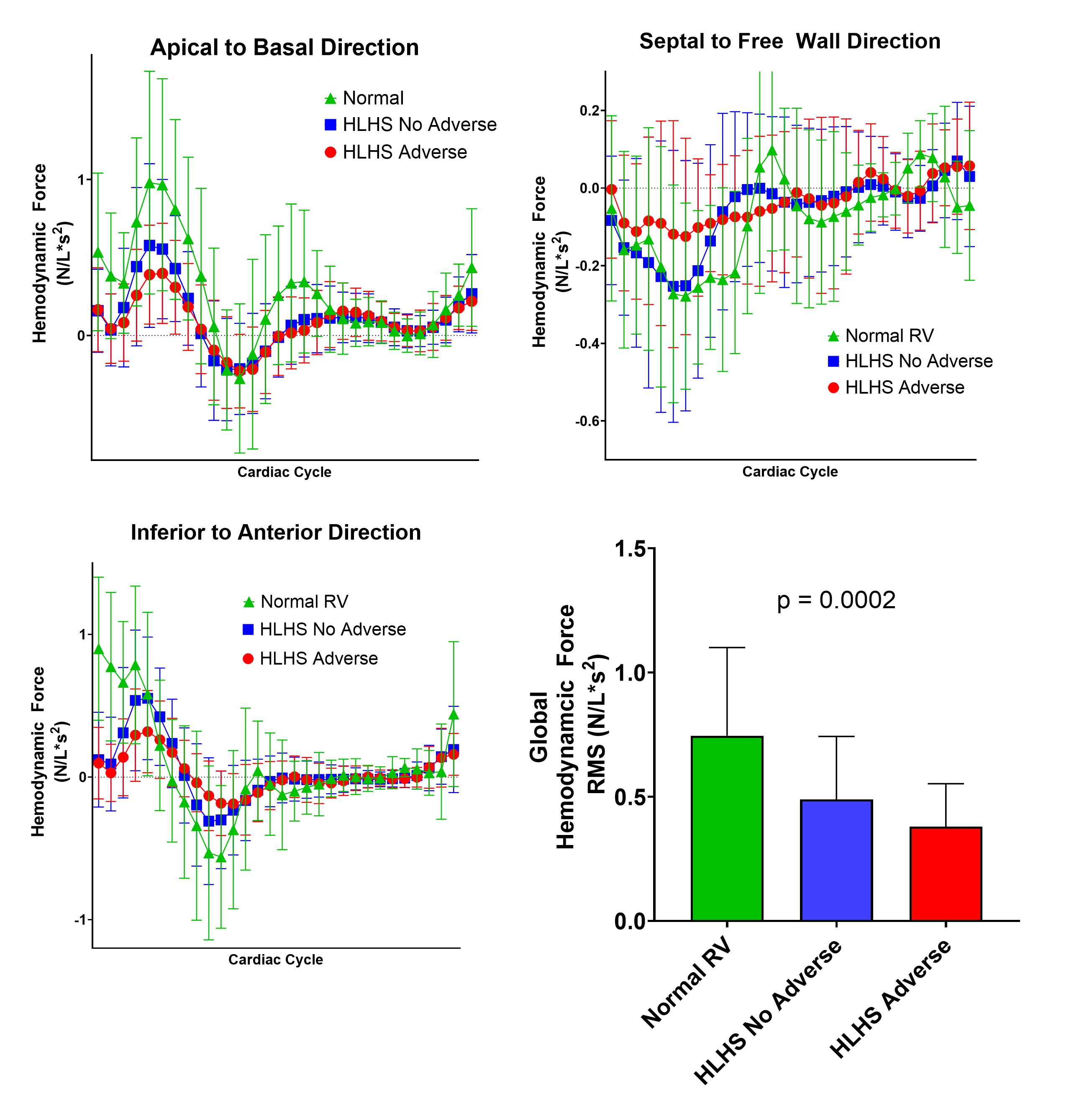
Forty-one HLHS patients (14%; 13.6±6.8 years, 33% female) had adverse outcomes with no differences in age/sex compared to those without adverse outcomes (14.8±6.4 years, 38% female). When compared to controls (14.2±5.4 years, 42% female), there was a reduction in systolic HDF along Apical-to-Basal axis (0.61±0.30 vs.0.84±0.34 N/L*s2, p=0.006) and increase in systolic HDF forces along Septal-to-Free Wall and Inferior-to-Anterior axis (0.42±0.28 vs. 0.28±0.15 N/L*s2, p< 0.0001; 0.86±0.37 vs. 0.36±0.21 N/L*s2, p< 0.0001 respectively). Lower HDF magnitude, increased RVEDVi and ≥moderate tricuspid regurgitation was associated with composite adverse outcomes on bivariable analysis (Table, Fig 2); of note, EF was not different between groups, although lower GCS trended towards adverse outcomes (p=0.08).
Conclusion:
HDF analysis of the systemic RV can be derived from CMR imaging. The systemic RV demonstrates alterations in HDF patterns when compared to the normal RV, and attenuation in systolic HDF magnitude is associated with adverse outcomes. HDF analysis could potentially determine subclinical progression of heart failure in HLHS patients and may be more sensitive than EF/GCS.
Figure 1 Caption – Methodology for hemodynamic force (HDF) analysis in hypoplastic left heart syndrome. The data contour points derived from feature strain tracking are used to deform the 3D model of the RV (left) to generate the overall RV kinematics. The endocardial wall motion is used to calculate the global HDF vector and its three components along a properly defined reference frame.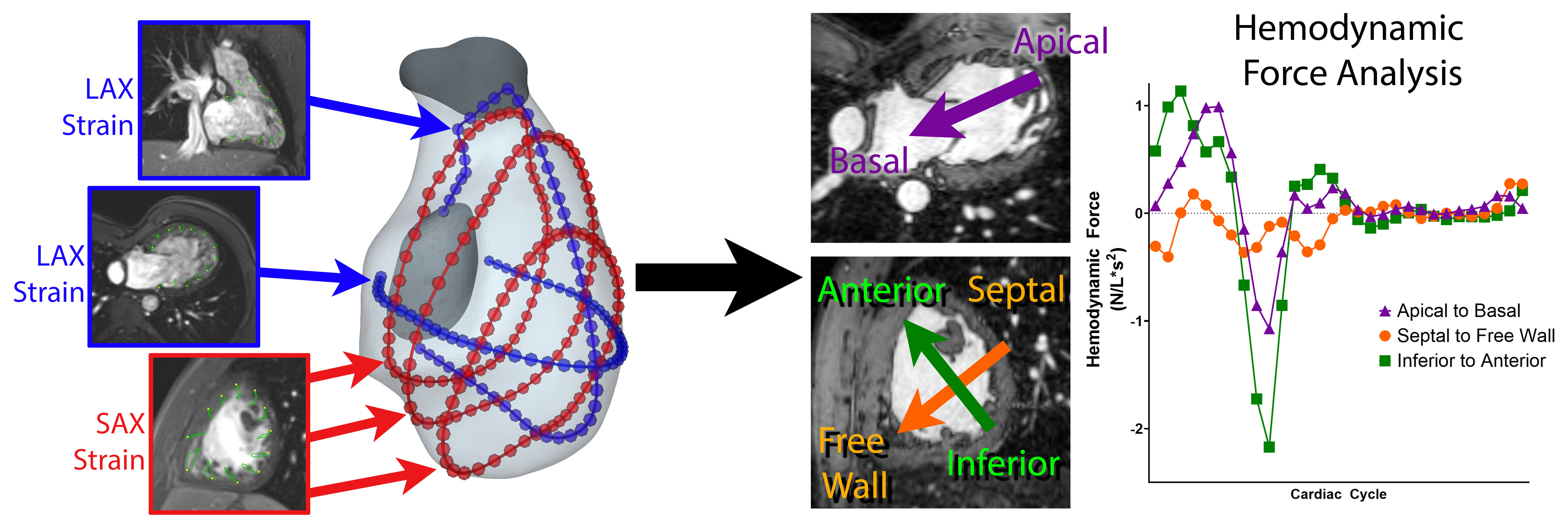
Figure 2 Caption – HDF temporal curves of the systemic RV and normal RV. The global HDF (root mean square/RMS over the entire cardiac cycle) is highest in the normal RV and lowest in HLHS patients with adverse outcomes.