
Rapid Fire Abstracts
Sarah E. Kollar, DO
Advanced Imaging Cardiologist
Children's National Hospital
Sarah E. Kollar, DO
Advanced Imaging Cardiologist
Children's National Hospital
Nicholas Mouzakis, RT
MR Technologist
Children's National Hospital
Jessica Lamartiniere, MRT
Cardiac MRI Technician
Children's National Hospital
Michelle Udine, MD
Advanced Imaging Cardiologist
Children's National Medical Center
Ravi Vamsee Vegulla, MD
Assistant Professor of Pediatrics
Children's National Medical Center
Seiji Ito, MD
Children's National Medical Center
.jpg "Uyen Truong, MD photo")
Uyen Truong, MD
Associate Professor
Children's National Hospital

Yue-Hin Loke, MD
Associate Professor
Children's National Medical Center
Cardiac magnetic resonance (CMR) of neonates with congenital heart disease (CHD) can be challenging due to the complex intracardiac flow features involved in CHD. 4D flow CMR offers the strong potential for comprehensive hemodynamic assessment of the whole heart. The use of ferumoxytol contrast significantly enhances the SNR of 4D flow which can be leveraged to address the relatively higher requirements of spatiotemporal resolution for small neonates/infants. We report our single center clinical and logistical experience on the use of ferumoxytol contrast-enhanced CMR in the assessment of small neonates/infants with CHD.
Methods:
The database of CMR studies were queried for scans performed from 2022 to 2024 on patients with body surface area < 0.25m2. Comparison of contrast-to-noise ratio (CNR) and signal-to-noise ratio (SNR) was performed against 21 CMR studies from 2019 to 2021. The demographics, indications and CMR scan times were collated. The selected CMR studies were either performed under moderate sedation/general anesthesia or non-sedated with feed & bundle. Standard ferumoxytol contrast dose was 3-4mg/kg, infused over 15 minutes in the CMR preprocedural room with continuous nursing monitoring. Standard CMR assessment included MR angiography, whole heart Inversion Recovery 3D and 4D flow with lab standard parameters as demonstrated in Table 1.
Results:
Thirty patients (age 1.3 IQR 0.28 – 2.56 months; body surface area 0.21m2±0.02; 56% female) underwent successful ferumoxytol contrast-enhanced CMR. There were no critical safety events during contrast infusion or CMR scan. Twenty-one (70%) of the cases were performed under moderate sedation/general anesthesia and nine (30%) cases were performed as a feed and bundle. 4D flow could not be performed in 2 of the feed and bundle cases due to significant patient motion, although the MR angiography provided adequate diagnostic information (vascular ring assessment). The remaining scans otherwise provided adequate structural and flow assessment of the anatomy (Figure 1). The overall scan time was 37±15 minutes and 4D flow scan time was 8±2 minutes. The average CNR was 142±55 and the average SNR was 156±57. Compared to prior years (2019-2021), the average CNR was 120±65 (p = 0.203) and SNR 131±72 (p = 0.178) amongst 21 patients with an average BSA of 0.49±0.18 m2 (p < 0.001). These findings demonstrate preservation of image quality despite scanning patients with significantly smaller BSA.
Conclusion: Ferumoxytol contrast enables the structural and functional assessment of CHD in small neonates/infants, particularly via the use of whole-heart 4D flow.
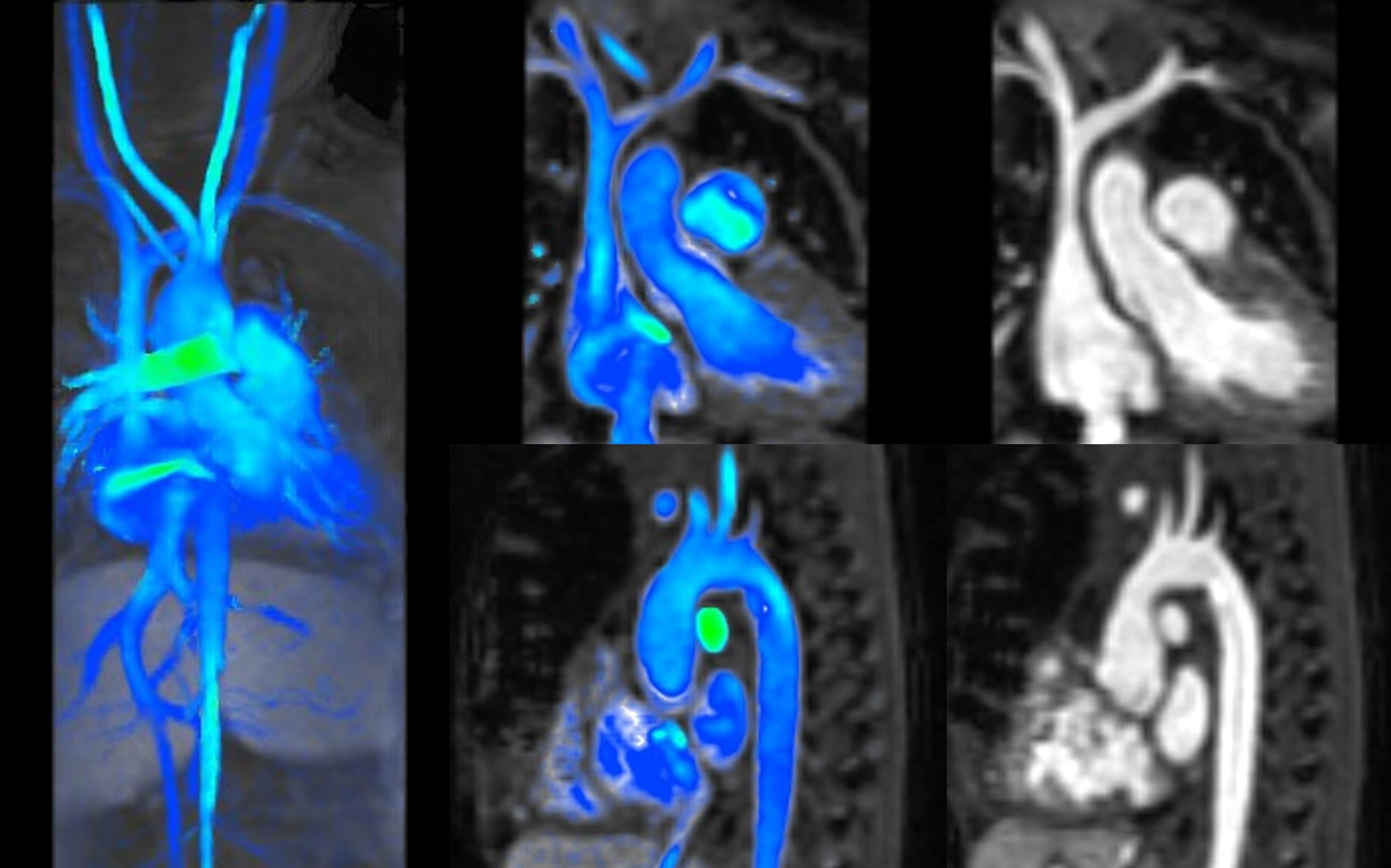
Figure 1: CMR study demonstrating 4D flow in a 2-month-old infant with a BSA of 0.16 m2 who underwent atrioventricular septal defect repair with residual left ventricle to right atrium shunt.
Figure 1: CMR study demonstrating 4D flow in a 2-month-old infant with a BSA of 0.16 m2 who underwent atrioventricular septal defect repair with residual left ventricle to right atrium shunt.
