Clinical & Translation

Manuel Morales, PhD
Instructor of Medicine
Beth Israel Deaconess Medical Center and Harvard Medical School
Manuel Morales, PhD
Instructor of Medicine
Beth Israel Deaconess Medical Center and Harvard Medical School
Jennifer Rodriguez
Clinical Trials Specialist
Beth Israel Deaconess Medical Center
Warren J. Manning, MD
Section Chief, Non-invasive Cardiac Imaging
Beth Israel Deaconess Medical Center/Harvard Medical School
Beth Israel Deaconess
Reza Nezafat, PhD
Professor
Harvard Medical School
Exercise cardiovascular magnetic resonance (Ex-CMR) real-time phase-contrast imaging enables flow quantification after physiological exercise. However, a tradeoff exists between spatial and temporal resolution. Insufficient temporal resolution limits Ex-CMR flow quantification during exercise. Therefore, we aimed to develop a deep learning model to increase real-time temporal resolution for Ex-CMR while maintaining spatial resolution.
Methods:
We developed a deformation encoding transformer (DENT) model for high-frame-rate flow imaging (Fig. 1) and applied it to a real-time flow sequence to achieve a 2-fold increase in temporal resolution and a 4-fold increase in framerate. The inputs are T = 4 velocity-compensated v0 or encoded v± images with temporal resolution Δt, acquired at times t - Δt, t, t + Δt and t + 2Δt. The output is an image interpolated in-between at t + 0.5Δt. DENT has six pairs of transformer layers whose inputs are split into windows along spatial and temporal dimensions. Spatiotemporal associations within windows were learned by applying self-attention to each window. These associations were used to predict non-rigid motion components, which were used to register the T frames to a single time point t + 0.5Δt. Breath-hold, 2D electrocardiogram (ECG)-gated flow images collected in multiple views from 1600 patients referred for clinical CMR were used for training. Velocity-compensated and encoded images with downsampled framerates were restored using DENT and compared to ground truth using L1 loss. In a prospective study of 12 patients referred for clinical CMR, a set of breath-hold, 2D ECG-gated flow for comparison and set of free-breathing, 2D real-time velocity-encoded (two-sided: v-, v+) images were collected in the aortic view with resolution of 2.5 × 1.9 mm2 and 44 ms. In a prospective Ex-CMR study of 8 healthy subjects, real-time images were collected before and after exercise. Phase-contrast data were obtained from two-sided v± images using conventional and view-sharing methods [1,2], resulting in flow images with an actual 88 ms resolution and framerates of 11 fps and 23 fps (Fig. 1B). DENT 4-fold reconstruction provided a true 44 ms resolution with 46 fps framerate.
Results:
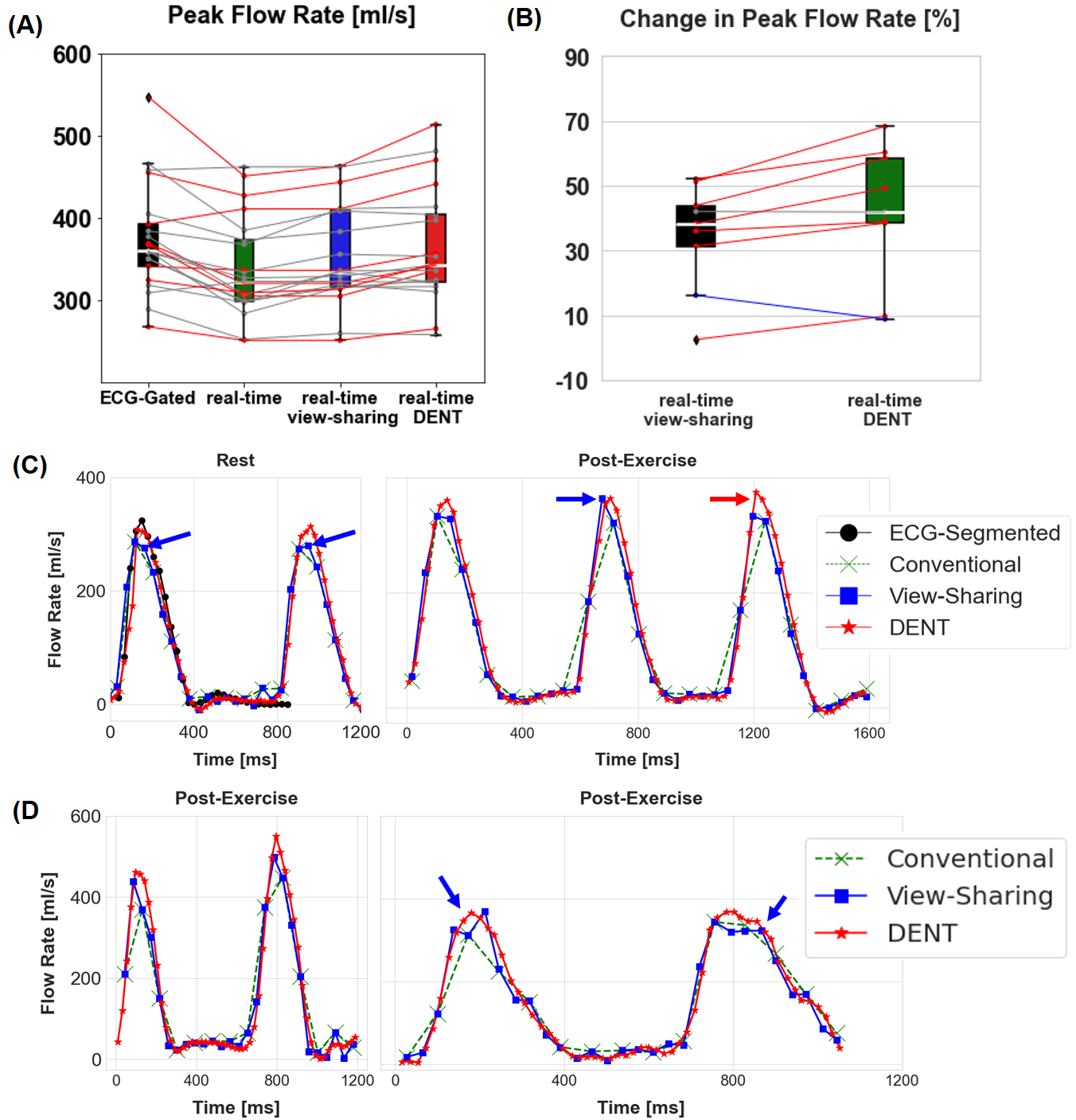
DENT removed flickering artifacts caused by view-sharing and improved quantification of flow (Fig. 2). Biases of peak parameters at rest (Fig. 3A) between ECG-gated and real-time flow (conventional, view-sharing, DENT): flow rate of -35 ± 30 ml/s, -22 ± 29 ml/s, -9 ± 3 ml/s; mean velocity of -8 ± 7 cm/s, -4 ± 5 cm/s, 2 ± 6 cm/s. (Fig.3B) View-sharing underestimated the change in peak flow rate post-exercise (42% vs 35%) relative to DENT, and in one case, inaccurately overestimated the change (Fig.3C). Representative subjects illustrating the benefit of DENT-based higher temporal resolution are shown in Fig.3D.
Conclusion:
DENT enabled a 4-fold gain in framerate and 2-fold gain in temporal resolution relative to conventional reconstruction, improving Ex-CMR flow measures.
Fig. 1 (A) DENT uses four velocity-encoded image frames with Δt resolution to interpolate a frame in between. Encoding transformer layers extract spatiotemporal features. Deconvolutional layers predict non-rigid motion parameters, which are used to sample and combine the four frames to produce the new velocity frame. (B) Real-time phase-contrast data obtained with conventional reconstruction have an effective resolution of 2∆t and framerate 1/2∆t. View-sharing doubles the framerate to 1/∆t. DENT doubles both framerate and temporal resolution. Repeating this process (DENT 4-fold) before phase-contrast reconstruction would provide a 4-fold gain in framerate..png)
Fig. 2. (A) Imaging parameters for ECG-gated and real-time two-sided phase-contrast imaging. Real-time images had a compressed sensing rate of 9, yielding a temporal resolution of 44 ms. (B) Conventional reconstruction of phase-contrast images from velocity-encoded data resulted in a true temporal resolution of 88 ms. View-sharing doubled the framerate, while DENT improved both framerate and resolution. Flickering artifacts in view-sharing appeared as intensity variations in temporal profile (white arrow). (C) Aortic (AO) flow rate was similar at rest for both methods and increased post-exercise. View-sharing underestimated the post-exercise peak (red arrow)..png)
Figure 3. (A) Comparison of resting peak flow rate between ECG-gated and real-time flow with conventional, view-sharing, and DENT methods (Fig. 1B). Conventional reconstruction produces one phase-contrast image for every velocity-encoded negative and positive pair (Fig. 1B). Red and blue lines indicate at least a 5% difference between view-sharing and DENT. (B) Changes in peak flow parameters after exercise. As shown in C, the single blue line reflects view-sharing's underestimation at rest (blue arrows) but not during exercise (blue and red arrows), which results in an exaggerated pre- and post-exercise change that is not real. (D) Representative subjects highlight the benefit of using DENT instead of view-sharing reconstruction.