
Rapid Fire Abstracts
Wouter J van Genuchten, MD, Msc
PHD candidate
Erasmus MC, Netherlands
Wouter J van Genuchten, MD, Msc
PHD candidate
Erasmus MC, Netherlands
Pablo Lamata, PhD
Professor
King’s College London, United Kingdom
Anna Zaske, BSc
Medical student
Erasmus MC, Netherlands
Zina Fejzic, MD
Pediatric cardiologist
Radboud UMC, Netherlands
Martijn Kauling, MD
Congenital cardiologist
Erasmus MC, Netherlands
Eric Boersma, PhD, MSc
Professor of Epidemiology
Erasmus MC, Netherlands
Miranda Snoeren, MD
MD
Radboud University Medical Center, Netherlands

Alexander Hirsch, MD, PhD, FSCMR
Cardiologist
Erasmus MC, Netherlands
Arend van Deutekom, MD, PhD, MSc
Pediatric Cardiologist
Erasmus MC, Netherlands

Willem A. Helbing, MD, PhD
Pediatric Cardiologist
Erasmus MC, Netherlands
Reduced exercise performance is common in patients with repaired tetralogy of Fallot (rToF), and relates to adverse outcomes. The effects of high-intensity interval training (HIIT) on exercise capacity and cardiac structure in rToF are unknown. We aimed to evaluate the feasibility, safety and effects of a home-based online-monitored HIIT programme on exercise capacity and cardiac structure in patients with rToF.
Methods:
A total of 34 patients with rToF aged 12-30 years (median age 16, IQR 14-23) were randomized to a 12-week home-based HIIT program or standard of care (SoC). The HIIT group performed three 30-minute sessions per week, with heart rate tele-monitoring. SoC involved exercise as usual. Primary endpoints were changes in peak oxygen consumption (VO2) and maximum workload. Secondary endpoints included MRI-derived measures of cardiac structure and function, including assessment of 3D cardiac anatomy using statistical shape models (SSMs). The SSMs of the patients with rToF were compared with those of age- and sex-matched healthy individuals (N = 26).
Results:
Following the HIIT intervention, peak VO2 increased from 36.0±7.9 ml/kg/min to 38.4±8.9 ml/kg/min (∆ 3.9 ml/kg/min (95% CI 2.1-5.7), Figure 1) and maximum workload increased from 202±56 watts to 219±58 watts (∆ 21 watts, (95% CI 10 – 28), Figure 1). No serious adverse events occurred. No changes in cardiac volumes or ejection fraction were observed after HIIT. In the SSM analyses, 14 modes captured over 80% of the population's right ventricular (RV) shape variability. The third mode (7.5 % of the variance) showed significant changes after HIIT (p = 0.01, figure B). Specifically, the RV septum exhibited increased short-axis curvature, and the overall RV assumed a more upright position., indicative of remodeling of towards a more normal shape of the volume overloaded RV. However, this change in mode 3 did not align RV morphology in rToF patients with that of healthy controls suggesting that this mode reflects a distinct, alternative adaptive remodeling trajectory in the rToF population.
Conclusion:
Home-based, online-monitored HIIT significantly improves exercise capacity in adolescents and young adults with rToF, without adverse effects on cardiac structure or function. Furthermore, HIIT led to remodeling of the right ventricle towards a more normal shape. The clinical implications of this remodeling remain to be determined. This study supports the feasibility and efficacy of home-based HIIT as a viable alternative to traditional supervised exercise programs for patients with rToF.
Figure 1: effects of HIIT on exercise capacity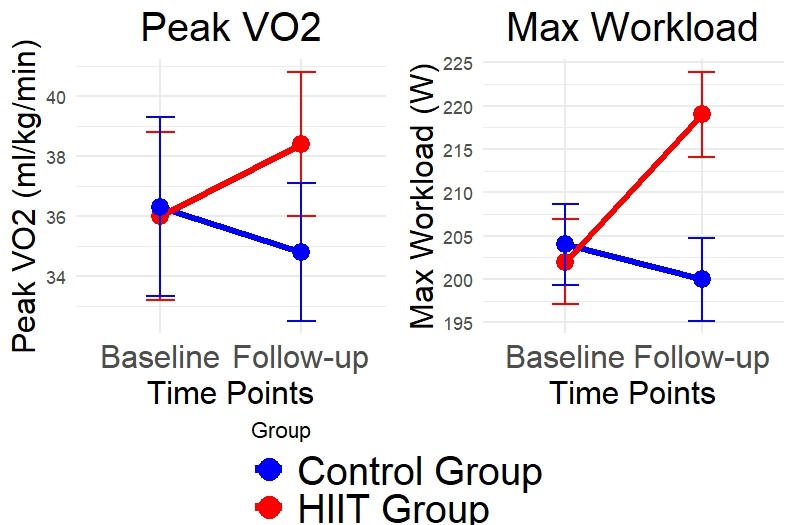
Figure 2: effects of HIIT on RV shape analyzed using SSM (mode 3)
