Oral Abstract

Theo Pezel, MD, PhD
Cardiologist
Hôpital Lariboisière – APHP, Paris, France, France

Trecy Gonçalves, MD
Cardiologist
Lariboisière Hospital – APHP, Paris, France., France
Solenn Toupin, PhD
Clinical scientist
Siemens Healthineers, France
Suzanne DUHAMEL, MD
Cardiologist
Institut Cardiovasculaire Paris Sud, France
Francesca Sanguineti, MD
Cardiologist
Institut Cardiovasculaire Paris Sud, France
Thierry Unterseeh, MD
Cardiologist
Institut Cardiovasculaire Paris Sud, France
Thomas Hovasse, MD
Cardiologist
Institut Cardiovasculaire Paris Sud, France
Alexandre Unger, MD
Cardiologist
Hôpital Lariboisière AP-HP, France
Jeremy FLORENCE, MD
Cardiologist
Lariboisière hospital, APHP, Paris, France., France
Jean Guillaume Dillinger, MD, PhD
Cardiologist
Lariboisière Hospital – APHP, Paris, France., France
Valérie Bousson, MD, PhD
Radiologist
Lariboisière Hospital – APHP, Paris, France., France

Jerome Garot, PhD
Head
ICPS - Massy, France
The presence and extent of late gadolinium enhancement (LGE) assessed by cardiac magnetic resonance imaging (CMR) are strong prognosticators of death in patients with non-ischaemic dilated cardiomyopathy (DCM), defined by the current guidelines as left ventricular (LV) dilation and left ventricular ejection fraction (LVEF)< 50%. Although the current guidelines defined the concept of “isolated LV dilation” as LV dilation with preserved LVEF≥ 50%, the prognostic value of the “LGE granularity” including its extent, location and pattern is not established in this population.
The aim of the study was to assess the prognostic value of the concept of “LGE granularity” including its extent, location, and pattern for predicting all-cause death above traditional prognosticators in patients with LV dilation and reduced LVEF (i.e. DCM) or preserved LVEF (i.e. isolated LV dilation), separately.
Methods:
Between 2008 and 2021, all consecutive patients with DCM and isolated LV dilation without ICD or history of sustained ventricular arrhythmia referred for CMR were included in two centres. All patients with history of coronary artery disease or myocarditis were excluded. The primary outcome was all-cause death using the French National Registry of Death. A 1:1 propensity score matching was performed to balance baseline characteristics in patients with DCM vs. those with isolated LV dilation. Cox regressions were performed to determine the prognostic value of each LGE findings.
Results:
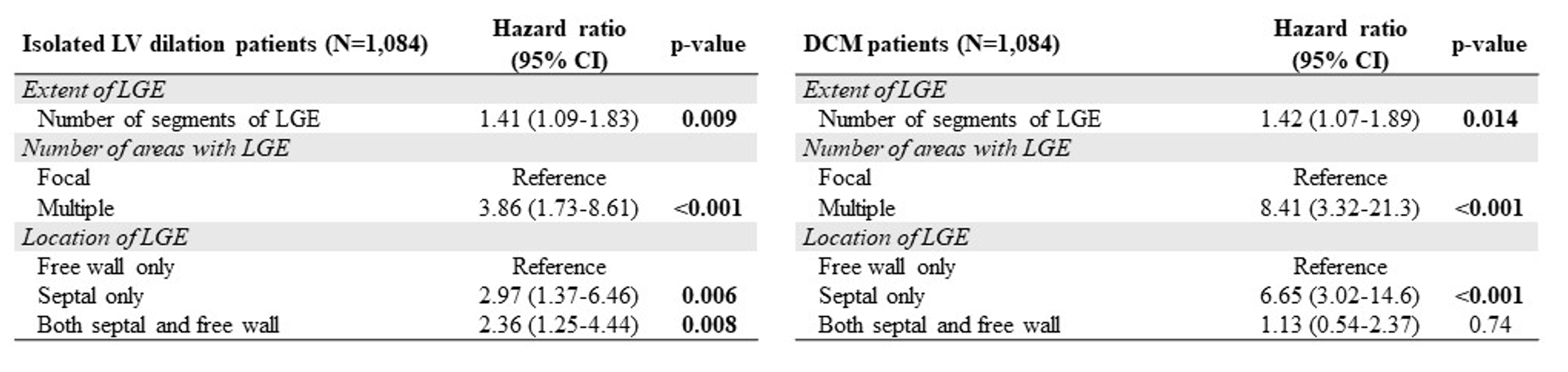
Of 2,752 patients analysed (age 52±8 years, 56% male), 408 (15%) patients died after a median (interquartile range) follow-up of 9 (7-12) years. A total of 737 (27%) patients had LGE. Patients with DCM had a higher rate of death than patients with isolated LV dilation (16% versus 13%, p=0.02). In the propensity-score matched population (N=1,084 in DCM subgroup and N=1,084 in isolated LV dilation), the LGE presence was associated with death (HR=2.98, 95%CI: 1.97-4.50, p< 0.001). In isolated LV dilation patients with LGE (N=265), the LGE extent (HR=1.41, 95%CI:1.09-1.83, p=0.009), the presence of LGE in multiple areas (HR=3.86, 95%CI: 1.73-8.61, p< 0.001) and the septal location (HR=2.97, 95%CI:1.37-6.46, p=0.006) were strong prognosticators of death after adjustment for traditional prognosticators. Similarly, in DCM patients with LGE (N=268), the LGE extent (HR=1.42, 95% CI:1.07-1.89, p=0.014), the presence of LGE in multiple areas (HR=8.41, 95%CI: 3.32-21.3, p< 0.001) and the septal location (HR=6.65, 95% CI: 3.02-14.6, p< 0.001) were strongly associated with death after adjustment.
Conclusion:
In a large cohort of DCM and isolated LV dilation patients, the concept of “LGE granularity” was independently associated with all-cause death after adjustment for all traditional prognosticators in both DCM and isolated LV dilation. These results suggest the existence of a continuum between isolated LV dilation and DCM, and that CMR assessment could improve the risk stratification in this population.
Survival curves of all-cause death in DCM and isolated LV dilation (ILVD) patients with LGE (N=737) 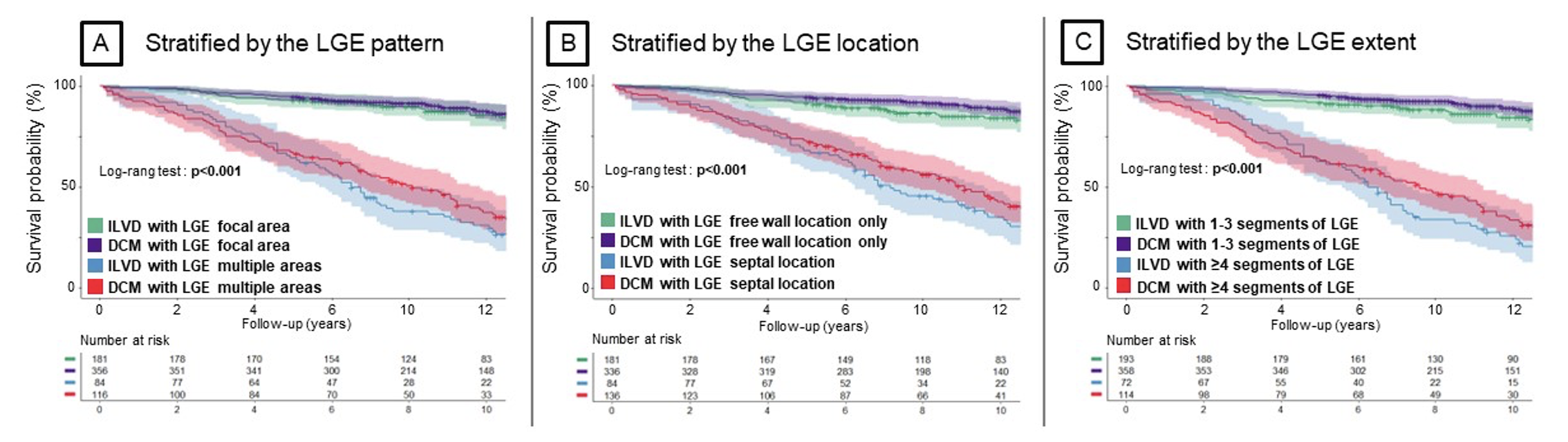
Multivariable analysis for the “LGE granularity” in 1:1 propensity-score matched population.