Oral Abstract
Yifan Wang, BSc
Medical Student
University of Ottawa, Canada
Yifan Wang, BSc
Medical Student
University of Ottawa, Canada
Justin J. Tse, PhD, MSc, BSc
Research Associate
University of Calgary, Canada

Ahmed Abdelhaleem, MD
Advanced Cardiac Imaging Fellow
West Virginia University Heart & Vascular Institute
Steven Dykstra, PhD
PhD Student
University of Calgary, Canada
Sandra Rivest, RN
Research Coordinator
Libin Cardiovascular Institute; University of Calgary, Canada
Jacqueline Flewitt, MSc
Manager of Strategic Partnerships
Libin Cardiovascular Institute; University of Calgary, Canada
Yuanchao Feng, PhD
Senior AHS analyst
Libin Cardiovascular Institute; University of Calgary, Canada
Andrew G. Howarth, MD, PhD
Associate Professor
Libin Cardiovascular Institute; University of Calgary, Canada
Carmen P. Lydell, MD
Clinical Associate Professor
Libin Cardiovascular Institute; University of Calgary, Canada
Louis Kolman, MD
Clinical Assistant Professor
Libin Cardiovascular Institute; University of Calgary, Canada
Robert JH Miller, MD
Clinical Assistant Professor
Libin Cardiovascular Institute of Alberta, University of Calgary, Canada
Nowell Fine, MD, MSc
Cardiologist / Associate Professor
Libin Cardiovascular Institute of Alberta, University of Calgary, Canada

Dina Labib, MD, PhD, FSCMR
Associate Scientific Director, Personalized Diagnostics Program; Adjunct Assistant Professor
University of Calgary, Canada

James A. White, MD
Professor
Libin Cardiovascular Institute; University of Calgary, Canada
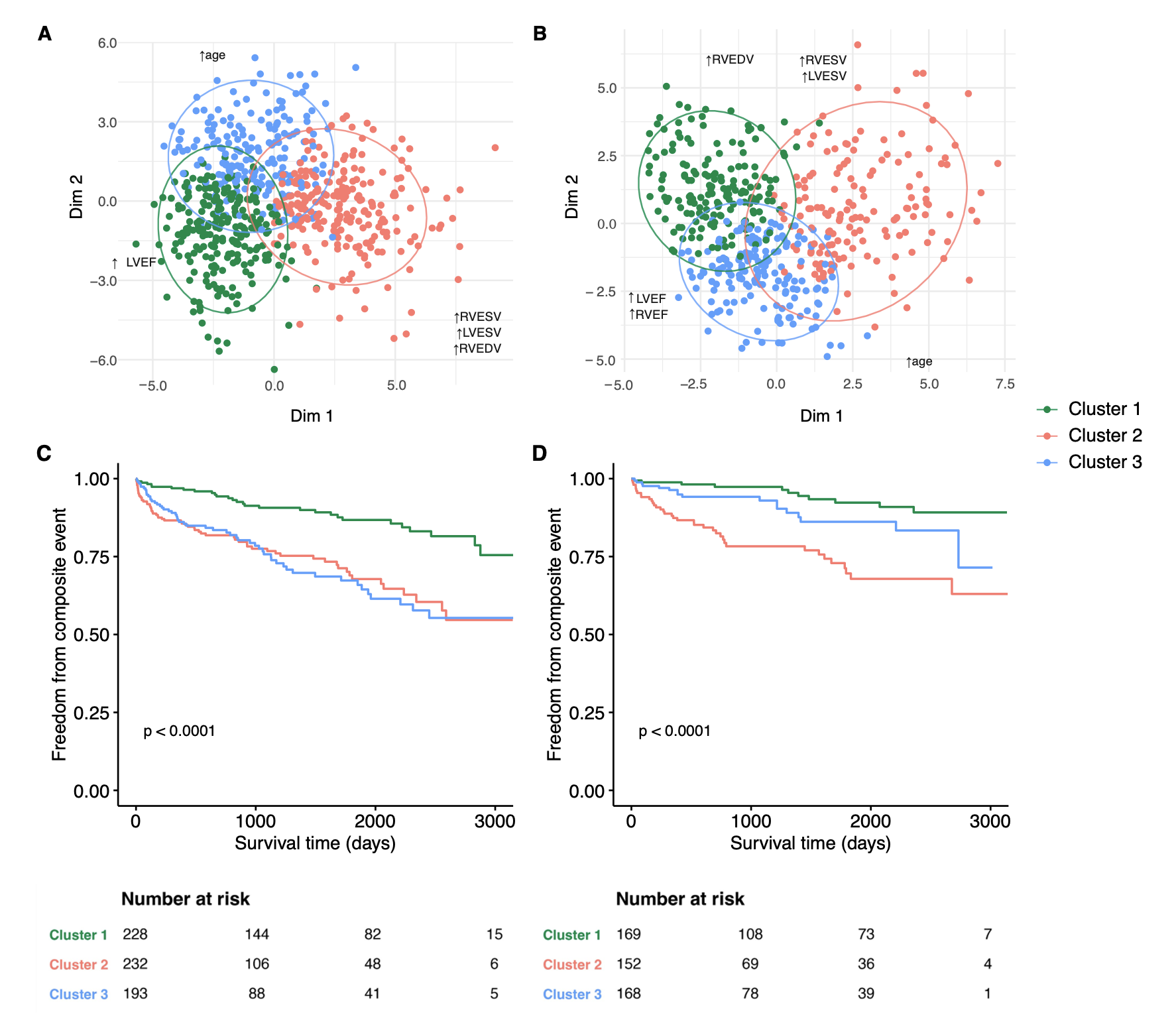
Three clusters were identified for both DCM and HNDC sub-cohorts, each demonstrating unique clinical and CMR characteristics (Tables 1 and 2). In both sub-cohorts, Cluster 1 was younger with mildly reduced LV EF. Cluster 2 exhibited worse clinical symptoms, higher loop diuretic usage, and severe LV systolic dysfunction with high fibrosis/scar burden. Cluster 3 was older with higher prevalence of comorbidities and moderate systolic dysfunction. In HNDC, Cluster 2 experienced a 4.7-fold increased risk of the composite outcome versus Cluster 1 (Figure 1; HR [95% CI] 4.7 [2.4-9.2]; p< 0.001), where-as a trend towards worse outcomes was observed for Cluster 3 (HR 2.0 [0.9-4.3]; p=0.07). In DCM, both Clusters 2 and 3 experienced a 2.8-fold increased risk of the outcome versus Cluster 1 (HR for each 2.8 [1.8-4.4]; p< 0.001).
Conclusion: Unsupervised phenotype clustering identifies high risk patients across both DCM and HNDC forms of NICM. This novel approach has the potential to improve capacity for the delivery of personalized care in patients with NICM.
Visualization of phenotype clusters in both the (A) Dilated cardiomyopathy (DCM) cohort and (B) Hypokinetic non-dilated cardiomyopathy (HNDC) cohort using factor analysis of mixed data (FAMD); Kaplan-Meier curves for freedom from composite outcome in both (C) DCM and (D) HNDC cohorts are shown based on cluster membership.