Oral Abstract

Alexander Schulz, MD
Dr.
Harvard Medical School / BIDMC, Germany
Alexander Schulz, MD
Dr.
Harvard Medical School / BIDMC, Germany

Amine Amyar, PhD
Instructor in medicine
Harvard Medical School - Beth Israel Deaconess Medical Center
Warren J. Manning, MD
Section Chief, Non-invasive Cardiac Imaging
Beth Israel Deaconess Medical Center/Harvard Medical School
Beth Israel Deaconess
Ethan Rowin, MD
Cardiologist
beth israel lahey health
Martin S Maron, MD
Cardiologist
beth israel lahey health
Reza Nezafat, PhD
Professor
Harvard Medical School
For asymptomatic patients with hypertrophic cardiomyopathy (HCM), early detection of heart failure (HF) to facilitate timely therapeutic interference remains challenging. In this study, we sought to identify distinct groups of asymptomatic HCM patients at risk of HF progression by applying an unbiased clustering approach using CMR and clinical features.
Methods:
Data of 377 asymptomatic (NYHA I) obstructive and non-obstructive HCM patients (49±16yrs, 26% female, 51% obstructive) who underwent CMR scans from 01/2002 to 04/2019 from 4 academic medical centers were included in the analyses. Most recent HF status was obtained up to January 11th 2022. HF progression was defined as a composite endpoint consisting of progression to NYHA ≥ II, or echocardiographic worsening of left ventricular (LV) ejection fraction < 50%. For an unbiased identification of distinct asymptomatic HCM phenotypes we implemented an unsupervised clustering algorithm(1). Twenty variables, including basic demographic information, HCM medication, known HF predictors, and indexed CMR-derived volumetric, functional, and quantitative late gadolinium enhancement (LGE) data, were chosen as input to the clustering model (Table 1). Before clustering, a distance matrix was computed to determine the distances between mixed typed data. Details of data preparation are shown in Fig 1. A K-Medoids(2) clustering algorithm calculated medoids (individual data points) as the cluster's center, with the goal of minimizing the distance between the medoids and all other data points within the same cluster. The optimal number of clusters was determined by evaluating the average Silhouette score of 2 to 10 clusters (Fig 1). Afterwards, outcome differences between the final clusters were investigated using Kaplan-Meyer plots and log-rank comparison. Cluster characteristics were compared using t-test and chi2-tests.
Results:
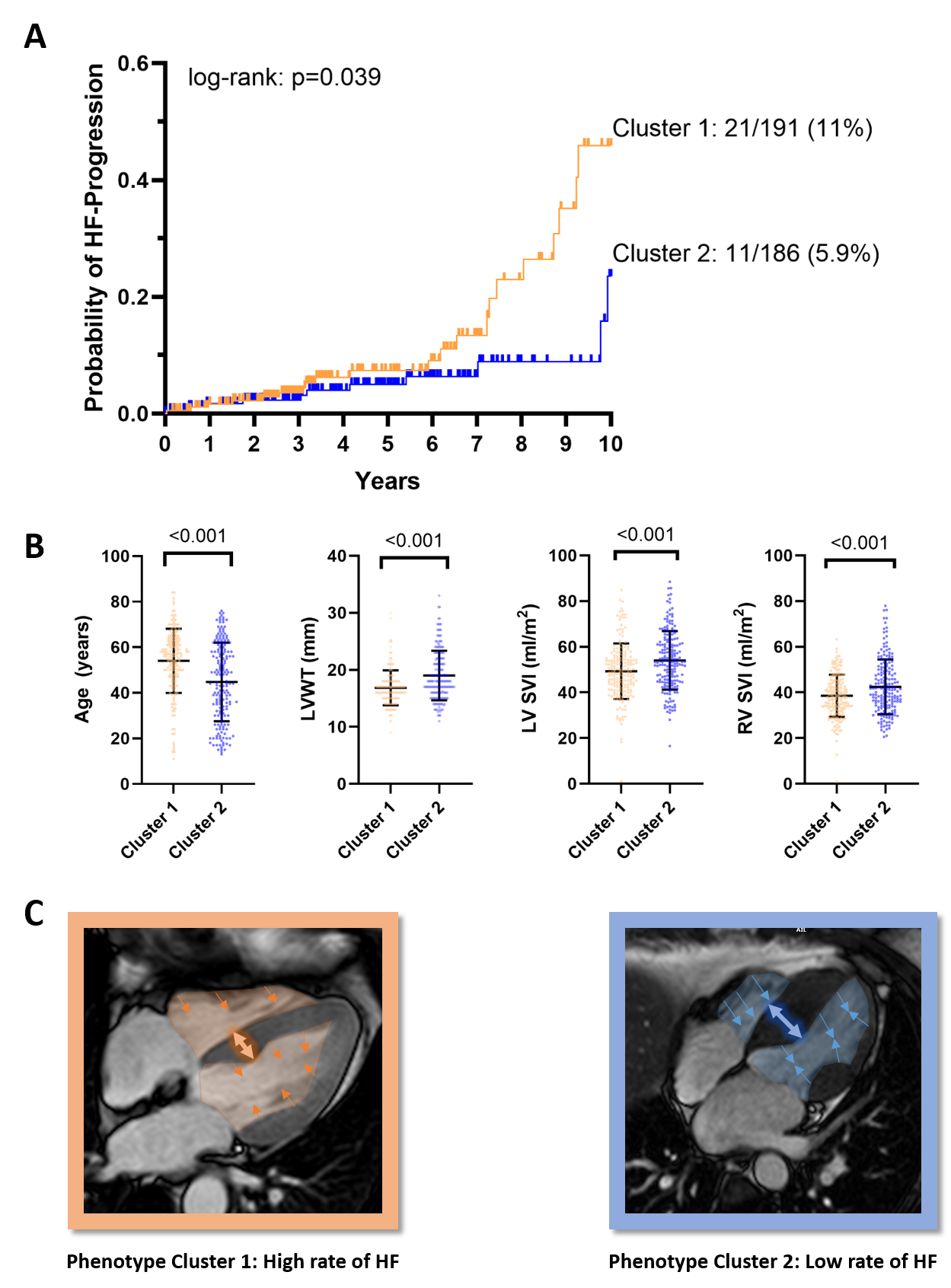
A total of 32 (8.5%) patients experienced HF progression during a mean follow-up of 4.4±2.6years. The K-Medoids revealed two distinct clusters of asymptomatic HCM patients based on the Silhouette score. Patients of Cluster 1 had a higher rate of long-term HF progression (Cluster 1: 21/191 (11%) vs. Cluster 2: 11/186 (5.9%), p=0.039) (Fig 2). Compared to Cluster 2, patients in Cluster 1, at risk of HF progression, were older but had comparable sex distributions, frequency of obstructive HCM, and apical hypertrophy (Table 1). Patients of Cluster 1 had less LV wall thickness, LV mass, and LGE, while biventricular stroke volumes and ejection fractions were impaired (Table 1).
Conclusion:
An unbiased clustering approach based on clinical and CMR metrics unravels a distinct group of asymptomatic HCM patients at higher risk of long-term HF progression. Characteristics of this group warrant further investigation to improve early prevention of heart failure.
Figure 1 Visualization of the unsupervised clustering process of mixed-type variables: After selecting 20 features, categorical variables are scaled using one-hot encoding and numerical variables using Min-Max normalization. Paired distances are calculated for both types individually, using Hamming distance for categorical and Euclidean distance for numerical variables. Average distances are stored in a distance matrix. An optimal number of clusters is defined using the Silhouette score, and unsupervised clustering is performed using K-Medoids clustering based on the precomputed distances. oHCM – obstructive hypertrophic cardiomyopathy, AFIB – atrial fibrillation, CC – calcium channel, LV – left ventricular, RV – right ventricular, EF –ejection fraction, EDVI – end diastolic volume index, ESVI –end systolic volume index, SVI –stroke volume index, LVMI – left ventricular mass index, LVWT – left ventricular wall thickness, LA – left atrium, LGE – late gadolinium enhancement.png)
Figure 2: Main characteristics of asymptomatic patients in Clusters 1 and 2: Row A shows as the Kaplan-Meyer-Plot indicating higher rates of long-term HF-Progression of patients in Cluster 1. Row B displays a graphical visualization of the main patient characteristics of both Clusters. Row C displays examples for CMR images of phenotypical patients of both clusters. The double arrows indicate the difference in LV mass. The inward pointing orange and blue arrows indicate differences in stroke volumes. LVWT – left ventricular wall thickness, LV SVI – Left ventricular stroke volume index, RV SVI – right ventricular stroke volume index, HF – heart failure