Oral Case
Maria-Daniela Valderrama-Achury, MD
Fellow Research Assistant
Research Institute Mcgill University Health Centre , Canada
Maria-Daniela Valderrama-Achury, MD
Fellow Research Assistant
Research Institute Mcgill University Health Centre , Canada
Daniela Torres, MD
Research assistant
LaCardio, Colombia
Julian Forero, MD
Radiologist
Fundacion CardioInfantil - Instituto de cardiologia, Colombia

Carlos Guerrero, MD
Adult Congenital heart Disease
Fundacion cardioinfantil-LaCardio
Bogota, Colombia
Jesus Agreda, MD
Cardiologist
Clínica Los Nogales, Colombia

Hector Medina, MD, MPH
Cardiac Imaging
Texas Heart Institute
Texas Heart
Michael Chetrit, MD
Assistant professor
McGill University Health Center, Canada
A 68-year-old female from Bogota, Colombia, had a trans-thoracic echocardiogram (TTE) done prior to cataract extraction surgery in December 2021, noticeable for regional wall motion abnormalities (RWMA) not following a coronary distribution. The patient was asymptomatic and had no prior medical of familial history of coronary disease or heart failure. General and cardiovascular physical examination was unremarkable. She was referred to our institution for a cardiac MRI for further characterization.
Diagnostic Techniques and Their Most Important Findings:
CMR findings:
A CMR was performed on a 1.5 T scanner (Philips, Ingenia) using a standard heart failure protocol. The cine during steady-state free precession sequence demonstrated mild left ventricular systolic dysfunction with an left ventricular ejection fraction (LVEF) of 40% and dilated left ventricle (Indexed LV end-diastolic volume 155.7 ml/m2) in addition to aneurysms, thinning and dyskinesis of the basal-inferolateral, mid-inferior, and apical walls (Figure 1).
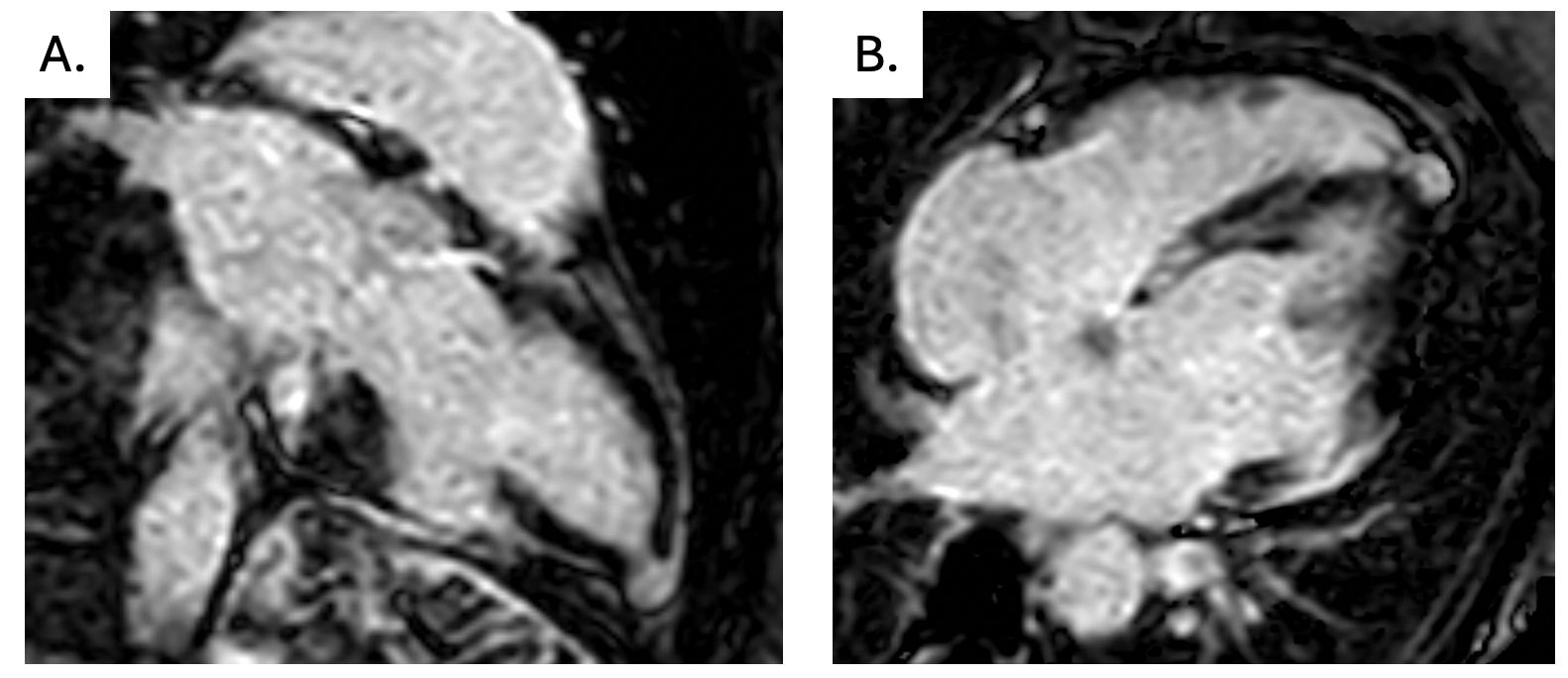
Late gadolinium enhancement (LGE) was performed 10 minutes post-contrast injection (0.15 mmol/kg, Gadobutrol) using a T1-weighted inversion recovery fast gradient echo sequence with an optimized inversion time. It demonstrated transmural enhancement matching the thinned and dyskinetic segments during SSFP’s. In addition, a left ventricular thrombus was noticed in the inferolateral aneurysm (Figure 2).
Considering these findings, serology was requested and confirmed the final diagnosis of Chagas Cardiomyopathy in an indeterminate, asymptomatic state. The patient was referred to a cardiologist to continue the follow-up and, at present time, the patient is still asymptomatic with functional class I.
Learning Points from this Case:
Ventricular aneurysms are a complication of Chagasic cardiomyopathy, typically described in the basal infero-lateral wall and the apex, although simultaneous aneurysm is not the most common presentation. Surprisingly, in this case, it was an incidental diagnosis and a clear example of an indeterminate stage diagnosed with a rare presentation of two simultaneous aneurysms, in addition to ventricular thrombi. Awareness of the Chagas Disease is crucial, detect anatomical changes in early stages is important to prevent progression and allows timely intervention.
Cardiac MRI (SSFP cine two-chamber, four-chamber, and LVOT view) showing 2 left ventricular aneurysms (inferolateral and apical). 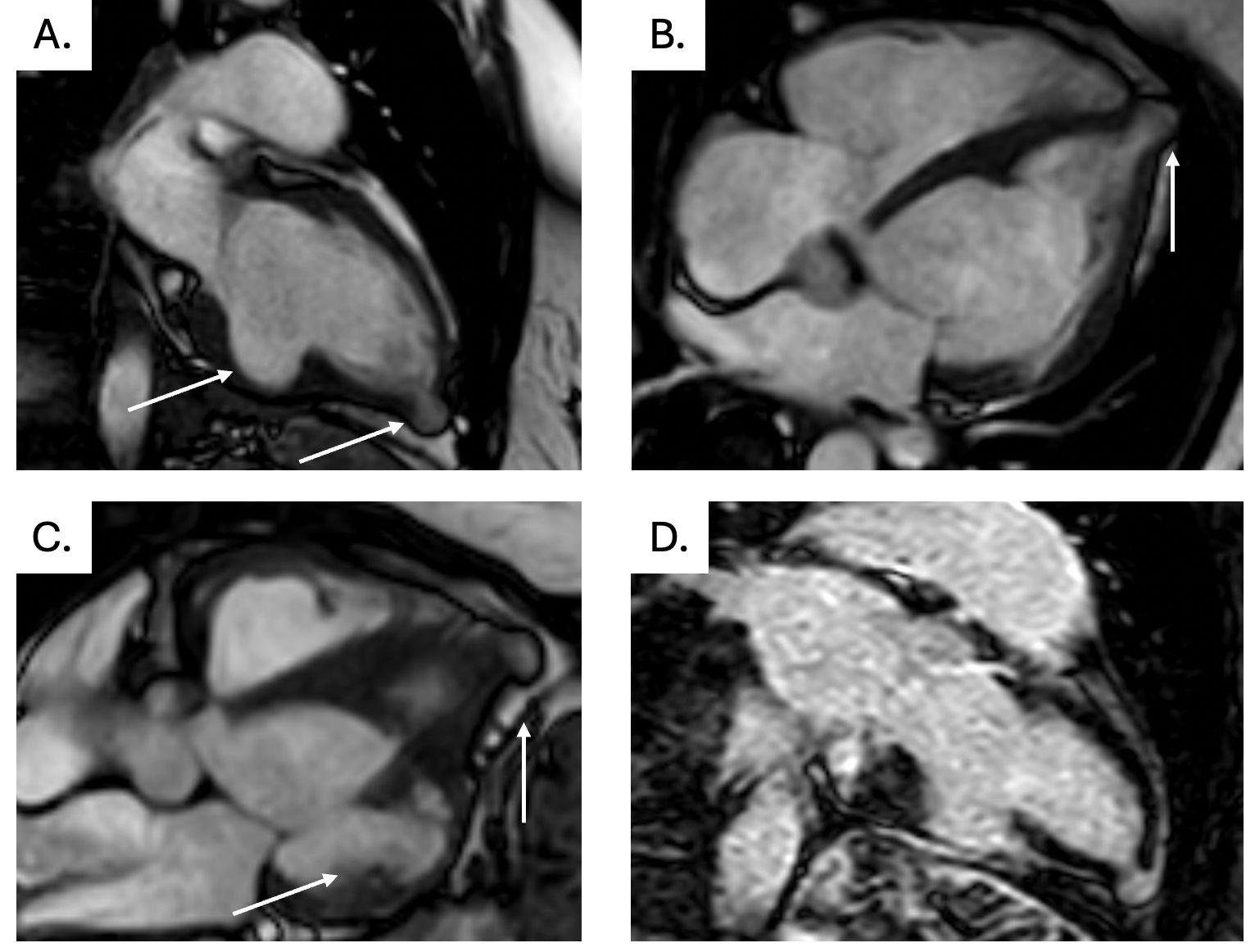
LGE sequences with an extensive trans-mural scar involving the inferolateral, and apical regions