Clinical & Translation
Ahsan A. Khan, MD
CMR Fellow
University of Calgary, Canada
Ahsan A. Khan, MD
CMR Fellow
University of Calgary, Canada

Dina Labib, MD, PhD, FSCMR
Associate Scientific Director, Personalized Diagnostics Program; Adjunct Assistant Professor
University of Calgary, Canada
Steven Dykstra, PhD
PhD Student
University of Calgary, Canada
Jacqueline Flewitt, MSc
Manager of Strategic Partnerships
Libin Cardiovascular Institute; University of Calgary, Canada
Sandra Rivest, RN
Research Coordinator
Libin Cardiovascular Institute; University of Calgary, Canada
Yuanchao Feng, PhD
Senior AHS analyst
Libin Cardiovascular Institute; University of Calgary, Canada
Andrew G. Howarth, MD, PhD
Associate Professor
Libin Cardiovascular Institute; University of Calgary, Canada
Carmen P. Lydell, MD
Clinical Associate Professor
Libin Cardiovascular Institute; University of Calgary, Canada
Louis Kolman, MD
Clinical Assistant Professor
Libin Cardiovascular Institute; University of Calgary, Canada
Jonathan Howlett, MD
Clinical Professor
University of Calgary, Canada
Robert J.H. Miller, MD
Clinical Assistant Professor
Libin Cardiovascular Institute; University of Calgary, Canada

James A. White, MD
Professor
Libin Cardiovascular Institute; University of Calgary, Canada
CMR-derived left ventricular (LV) filling pressure (LVFPcmr) is a promising prognostic marker in patients with known or suspected heart failure, comparable to invasively measured values. However, studies to date assessing this marker were relatively small-sized studies, with some excluding patients with coronary artery disease (CAD). Little is known about the prognostic value of this marker in a broad cardiovascular disease referral cohort. We sought to explore the associations of LVFPcmr with future heart failure outcomes in a diverse CMR referral cohort identified from the Cardiovascular Imaging Registry of Calgary (CIROC).
Methods:
We analyzed consecutive adult patients enrolled in the Registry between 2015 and 2021. Subjects completed baseline patient-reported health questionnaires administered by tablet-based software (intakeDITM, Cohesic Inc., Calgary, AB), followed by CMR imaging with standardized reporting of disease phenotypes (cardioDITM, Cohesic Inc., Calgary, AB). Patients were followed for a minimum of 6 months for a composite outcome of heart failure mortality, heart failure hospitalization, cardiac transplantation, or LVAD implantation. LVFPcmr was calculated as: 6.1352 + 0.07204 * left atrial volume + 0.02256 * LV mass. Fine-Gray models were constructed to test associations of this marker with the primary outcome.
Results:
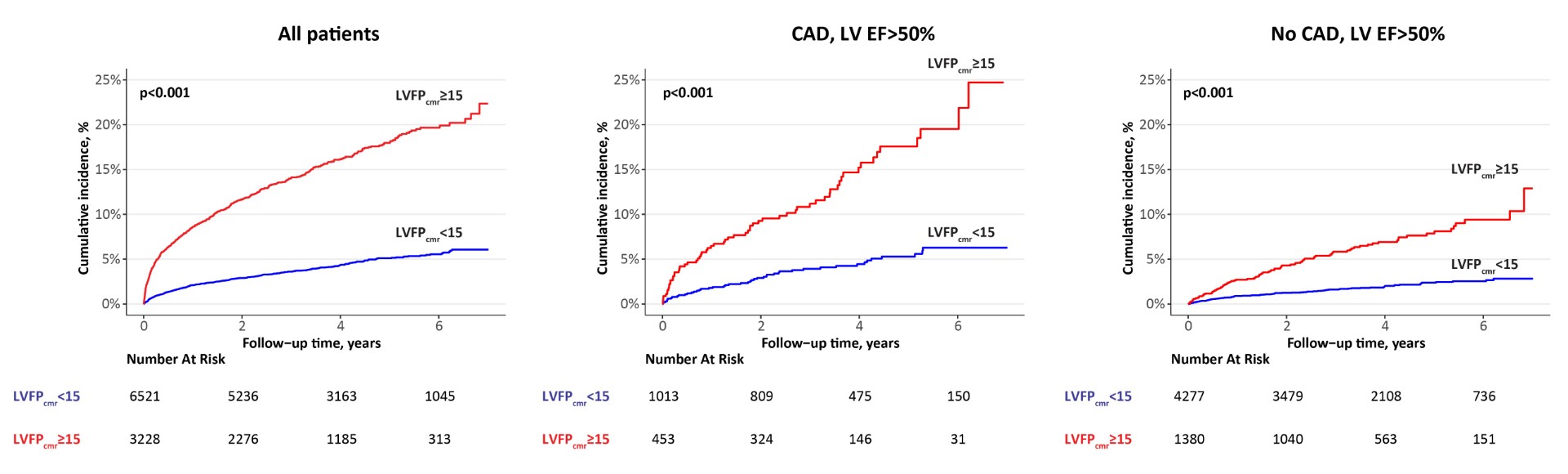
A total of 9,749 patients were analyzed (mean age 57 years, 62% male). Baseline characteristics of the study population are shown in Table 1. Over a median follow-up of 3.9 years, 783 patients (8%) experienced the primary outcome. LVFPcmr was significantly associated with the outcome after adjusting for clinically relevant variables (sub-distribution hazard ratio [HR] 1.14 per 1 mmHg; 95% CI 1.03-1.3; p=0.01; Figure 1). Using a survival-based approach, an optimal cut point of 15 mmHg for LVFPcmr was identified. LVFPcmr ≥the cut point had an adjusted HR 1.82 (1.45-2.28) for the outcome (p< 0.001) vs low LVFPcmr. We further explored the associations of dichotomized LVFPcmr with the outcome in subgroups of patients with and without history of CAD across 3 categories of LV ejection fraction (EF): < 40%, 40-50%, and >50%. In multivariable models, high LVFPcmr remained independently associated with the outcome in subgroups with and without CAD having an LV EF >50% (respective adjusted HR 2.92 [1.63-5.24] and 2.88 [1.77-4.67]; p< 0.001 for both). There were no significant associations in all other subgroups. Cumulative incidence plots for the overall cohort and the subgroups with an LV EF >50% are shown in Figure 2.
Conclusion:
In this largest study to date, assessing the prognostic value of LVFPcmr in a diverse CMR referral cohort, we identified LVFPcmr to be a powerful predictor of adverse outcomes in patients with preserved LV ejection fraction, inclusive of subgroups with and without CAD. This simple, non-invasive tool offers potential for risk stratification in patients with various cardiac diagnoses that are not restricted to a heart failure presentation.
Figure 1. Forest plot of association of LVFPcmr with the composite outcome, using a multi-variable Fine-Gray model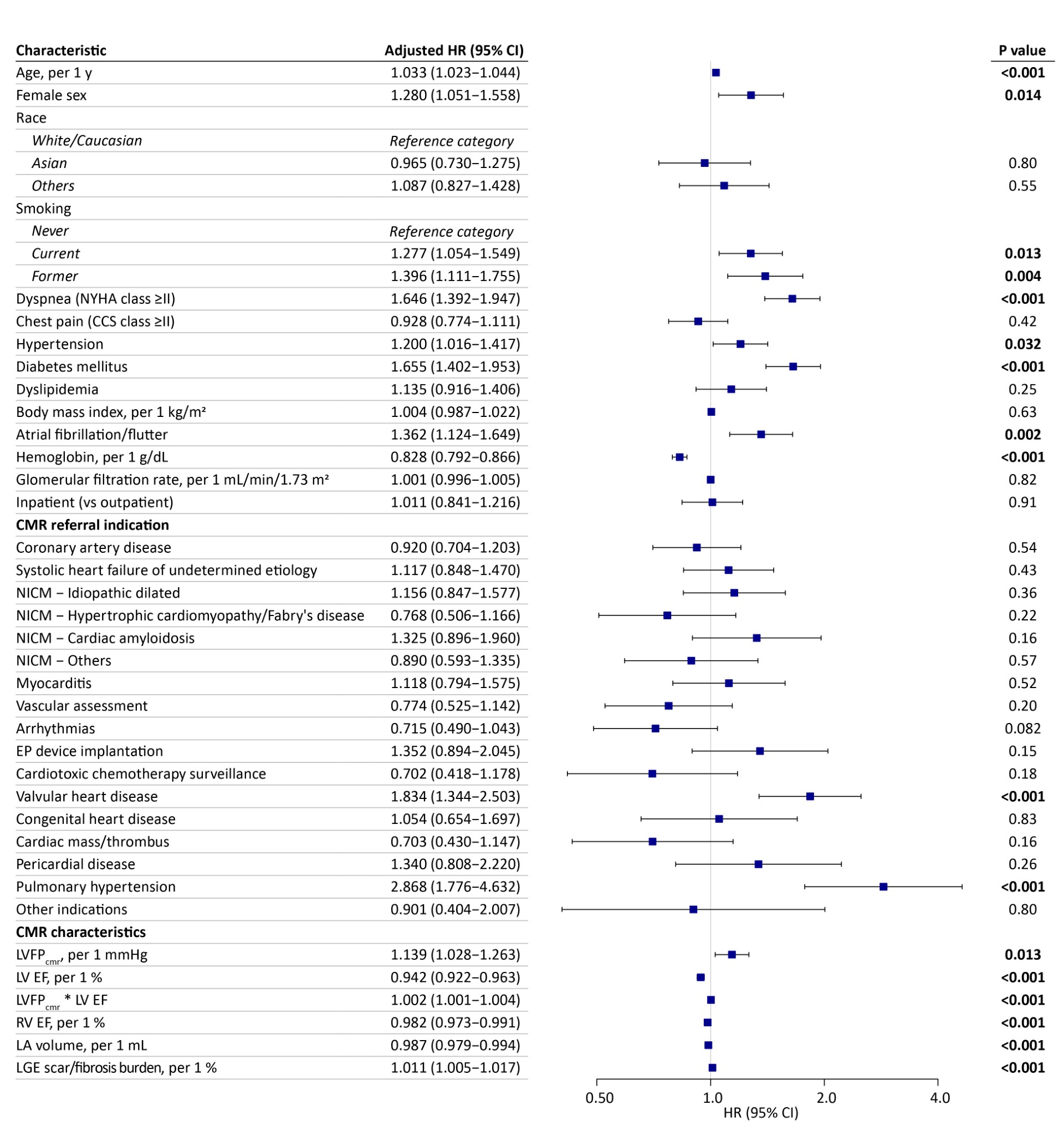
Figure 2. Cumulative incidence of the primary composite outcome for the categories of CMR-derived LV filling pressure (LVFPcmr) in the overall cohort, coronary artery disease and no coronary artery disease with an LV EF >50%