
Quick Fire Cases
Ian C. Chang, MD
Assistant Professor and Consultant
Mayo Clinic
Ian C. Chang, MD
Assistant Professor and Consultant
Mayo Clinic
A 24-year-old female was admitted for evaluation of syncope with a head injury. The patient reported a history of syncope that has been mostly unprovoked since she was 15 years old.
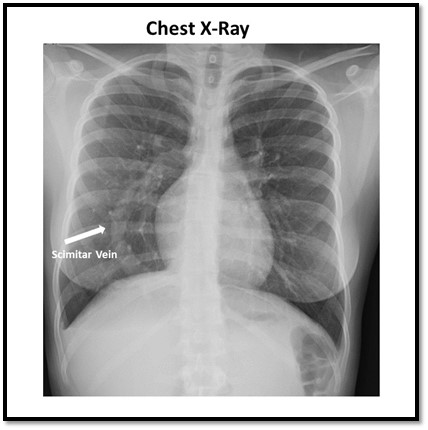
She was hypotensive (blood pressure: 89/63 mmHg) with a body mass index of 19.79 at the admission time. The remainder of the physical examinations and laboratory values were within normal limits. After further evaluation, a chest x-ray demonstrated the scimitar sign, suggesting a congenital partial anomalous right pulmonary venous return to the inferior vena cava (IVC) (Figure 1).
Diagnostic Techniques and Their Most Important Findings: Congenital partial anomalous pulmonary venous return (PAPVR) is a rare congenital heart disease defined as the drainage of one or more pulmonary veins to the systemic venous system, most commonly the right superior vena cava, instead of the left atrium. When the right pulmonary vein drains into IVC, it is known as scimitar syndrome. Scimitar syndrome also has associated right lung and pulmonary artery hypoplasia, dextrocardia, and an anomalous systemic blood supply to the right lung. Adults are often asymptomatic but may experience recurrent pulmonary infections or dyspnea on exertion.
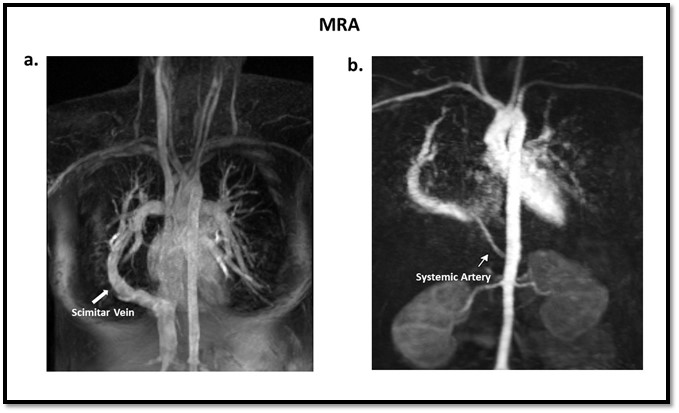
In this case, partial anomalous right pulmonary venous return to the IVC and also an anomalous systemic artery from the abdominal aorta to the right lung were identified (Figure 2). We did not observe dextrocardia or hypoplastic right pulmonary artery.
PAPVR leads to the shunting of blood from the systemic circulation to the pulmonary circulation, leading to volume overload of the right ventricle as well as pulmonary hypertension. Although PAPVR can be easily diagnosed with multi-modality imaging, accurately quantifying the severity of the shunt can be a challenge.
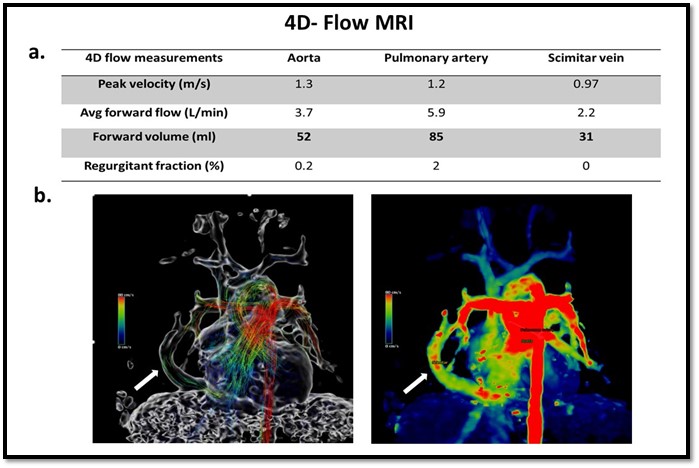
Four-dimensional (4D) flow MRI may be a useful non-invasive tool to evaluate the degree of shunt in patients with PAPVR or scimitar syndrome . Our 4D flow analysis calculated a systemic stroke volume of 52 ml and a pulmonary stroke volume of 85 ml. The flow through the scimitar vein was 31 ml, matching approximately the stroke volume difference between the pulmonary and systemic circulation (Figure 3). 4D flow MRI calculated a hemodynamically significant left-to-right shunt with a Qp/Qs = 1.6, suggesting that surgical intervention should be considered in this symptomatic patient.
Learning Points from this Case:
We showed that 4D flow MRI can be a potential non-invasive diagnostic technique to quantify the severity of left to right shunt in scimitar syndrome. Apart from measuring stroke volume, measuring flow disturbances such as vortical flow formation instead of laminar flow might be a diagnostic finding for future investigations.
Figure 1. The chest X-ray of our patient clearly showed the scimitar vein.
Figure 2. Magnetic resonance angiography (MRA) of our case clearly displays a. a scimitar sign, with an arrow indicating the scimitar vein, and b. an arrow showing a systemic artery arising from the abdominal aorta to supply the right lung.
Figure 3. 4D flow MRI was conducted to capture optimal flow patterns; a. summarized flow quantification measurements including peak velocity, average forward flow, forward volume, and regurgitant fraction. The difference between the stroke volume of the aorta and pulmonary artery is primarily attributed to the flow from the scimitar vein to the inferior vena cava; b. 4D flow images clearly display the flow streamlines with corresponding color bars.
Figure 1. The chest X-ray of our patient clearly showed the scimitar vein.
Figure 2. Magnetic resonance angiography (MRA) of our case clearly displays a. a scimitar sign, with an arrow indicating the scimitar vein, and b. an arrow showing a systemic artery arising from the abdominal aorta to supply the right lung.
Figure 3. 4D flow MRI was conducted to capture optimal flow patterns; a. summarized flow quantification measurements including peak velocity, average forward flow, forward volume, and regurgitant fraction. The difference between the stroke volume of the aorta and pulmonary artery is primarily attributed to the flow from the scimitar vein to the inferior vena cava; b. 4D flow images clearly display the flow streamlines with corresponding color bars.
