Oral Case
Anna Székely, MD
MD, PhD-student
Lund University and Skåne University Hospital, Sweden, Sweden
Anna Székely, MD
MD, PhD-student
Lund University and Skåne University Hospital, Sweden, Sweden
Anders Nelsson, MD
MD, PhD Student
Lund University and Skåne University Hospital, Lund, Sweden, Sweden
Peter Kellman, PhD
Director of the Medical Signal and Image Processing Program
National Heart, Lung, and Blood Institute, National Institutes of Health
Håkan Arheden, MD, PhD
MD, PhD, Professor
Lund University and Skåne University Hospital, Lund, Sweden, Sweden

Henrik Engblom, MD, PhD
Professor, MD
Clinical Physiology, Department of Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden, Sweden
A 62-year-old woman presented with increasing dyspnea over the last years. She had pulmonary sarcoidosis for over ten years, but no confirmed cardiac involvement. Coronary angiography two years ago showed borderline significant atherosclerosis in a diagonal branch. No revascularization was performed. Due to worsening dyspnea, she was referred for cardiac magnetic resonance (CMR) with quantitative first-pass perfusion (qFPP) mapping with adenosine stress. The evening before the examination she had a cup of coffee by mistake, despite instruction to abstain from caffeine for 24h.
Diagnostic Techniques and Their Most Important Findings:
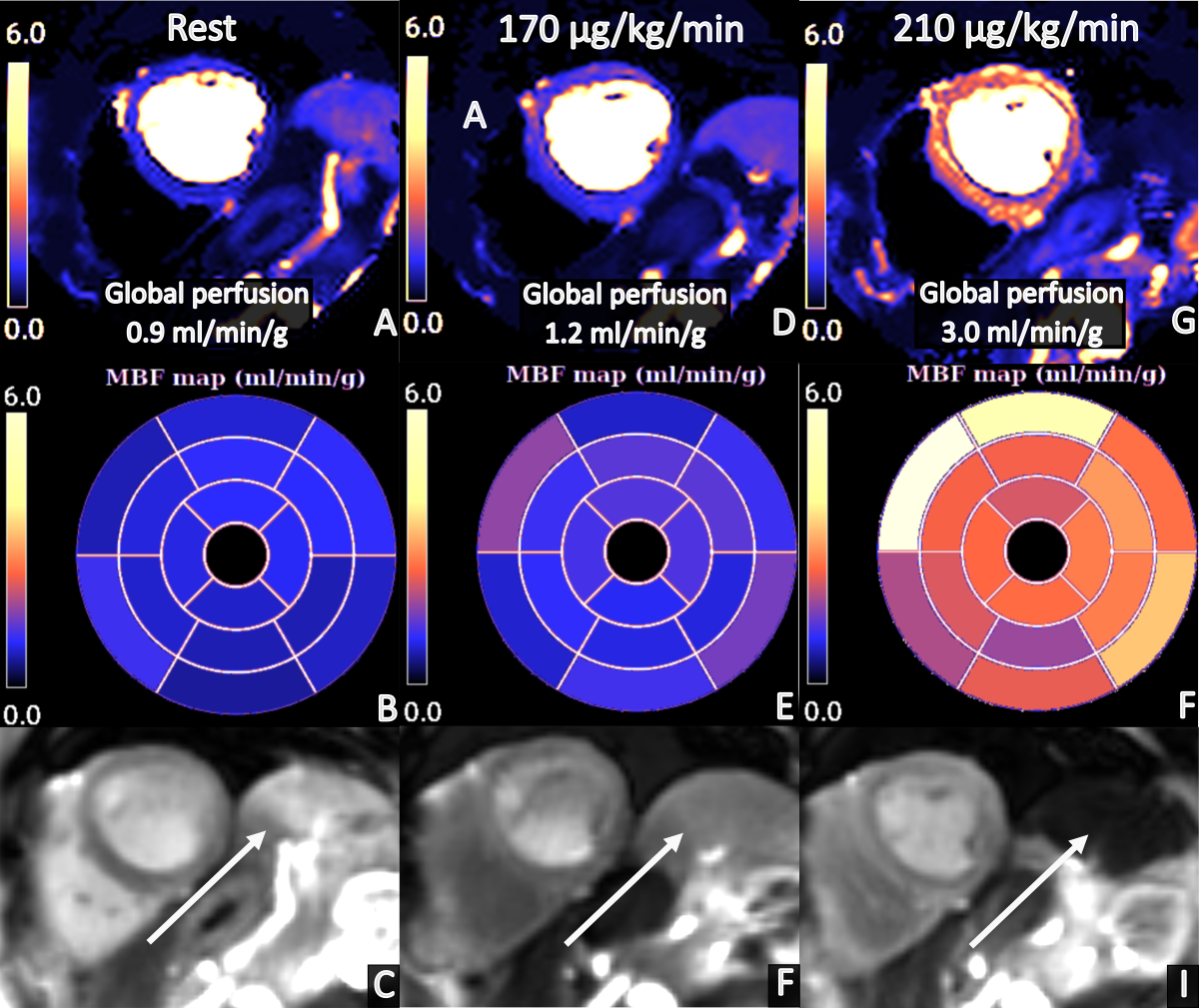
CMR with adenosine stress at standard dose (140 µg/kg/min) was initiated. No heart rate increase, blood pressure drop, or symptoms were registered after one minute of infusion. According to clinical protocol, the dose was increased to 170 µg/kg/min. Heart rate increased by 17 beats/minute and the patient experienced adenosine related symptoms. After two minutes of infusion of 170 µg/kg/min the perfusion images were acquired using a 1.5 T MR scanner (Siemens Magnetom Sola) and single-bolus dual-sequence perfusion mapping. Due to globally reduced myocardial perfusion (1.2ml/min/g) and no splenic switch off (Figure 1), absence of adenosine effect was suspected. Therefore, a new stress acquisition was performed in the same imaging session, now with an adenosine dose of 210 µg/kg/min from start showing normal global myocardial perfusion of 3.0 ml/min/g without regional ischemia (Figure 1). Global rest perfusion was 0.9 ml/min/g. Furthermore, the cine images revealed an ejection fraction of 40% and dilated ventricles, but the late gadolinium enhancement images showed no signs of cardiac sarcoidosis or infarction.
Learning Points from this Case:
Increased heart rate and blood pressure drop are poor predictors of achieved hyperemia during adenosine stress, yet these parameters are used in clinical practice to assess the adenosine response. In the current case, the absence of increased stress perfusion at an adenosine dose of 170 µg/kg/min could have been interpreted as three vessel disease or microvascular dysfunction. This poses an important clinical challenge, especially when using imaging modalities depicting relative perfusion distribution, such as myocardial scintigraphy or non-quantitative FPP, where absence of adenosine effect can mask a regional perfusion defect. Using qFPP CMR, the perfusion map and absence of splenic switch off can be used as an indicator of the adenosine effect. Intake of caffeine less than 24 hours before the examination motivates a more liberal increase of the adenosine dose to 210 µg/kg/min. Furthermore, reduced ejection fraction increases the likelihood of an inadequate adenosine response. To avoid misdiagnosing patients due to absence of adenosine effect, further studies of how adenosine should be dosed depending on patient specific factors are warranted.
Figure 1. The first column shows the perfusion map (A) and bulls eye plot (B) with global rest perfusion at 0.9 ml/min/g and absence of splenic switch off pointed by a white arrow (C). The second column shows the perfusion map (D) and bulls eye plot (E) with global stress perfusion at 1.2 ml/min/g and absence of splenic switch off pointed by a white arrow (F) acquired at an adenosine dose of 170 µg/kg/min. The third column shows the corresponding images at an adenosine dose of 210 µg/kg/min with global stress perfusion at 3.0 ml/min/g (G, F) and splenic switch off present (I).