Rapid Fire Abstracts
Anastasia Fotaki
Royal Brompton, UK
Anastasia Fotaki
Royal Brompton, UK
Carlos Castillo, MSc
PhD Candidate
King's College London, United Kingdom
Michael G. Crabb, PhD
Research Associate
King's College London, United Kingdom

Simon J. Littlewood, MBChB
Clinical Research Fellow
King's College London, United Kingdom
Karl P. P. Kunze, PhD
Senior Key Expert at Siemens Healthineers
King's College London, United Kingdom

Kuberan Pushparajah, MD, BMBS, BMedSc
Paediatric cardiology consultant
Evelina London Children’s Hospital/ King's College London, United Kingdom

Rene Michael M Botnar, PhD
Director and Professor
Institute for Biological and Medical Engineering
UC Chile, Chile

Claudia Prieto, PhD
Professor
Pontificia Universidad Católica de Chile / King's College London, United Kingdom
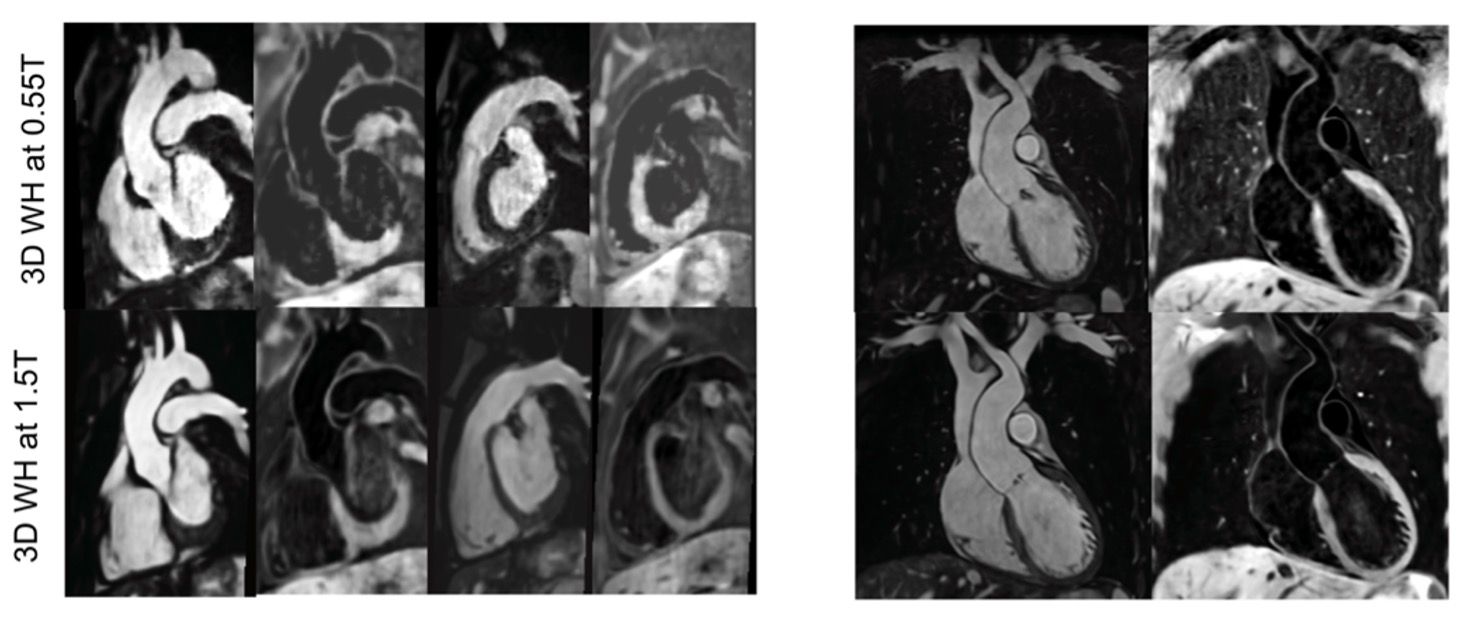
Low magnetic field systems provide an opportunity for affordable and accessible CMR to diverse clinical populations. 3D whole-heart imaging applications at low-field are limited [1]. A recently introduced sequence for bright- and black-blood magnetic resonance angiography (iT2Prep-BOOST) was modified to operate at 0.55T, in order to exploit state-of-the-art hardware [2]. In this study, we extend the comparison of this novel sequence to its 1.5T counterpart in adult patients with congenital heart disease (ACHD).
Methods:
ACHD patients underwent an ECG-triggered free-breathing 3D iT2prep-BOOST sequence acquired with an undersampled variable-density Cartesian trajectory [3], image-based navigation (iNAV) for respiratory and non-rigid motion correction and 3D-PROST denoising [4] at 0.55T (MAGNETOM Free.Max, Siemens Healthcare) and at 1.5T (Aera Siemens Healthcare). The parameters for 0.55T vs 1.5T were: 3D bSSFP readout, spatial resolution=1.5 mm3, flip-angle HB1/HB2 = 110/80 deg, FOV=312x312x120mm vs 400×300×104 mm, TR/TE:5.3/2.65 vs 3.24/1.41 ms bandwidth = 800 Hz/px vs 930 Hz/px respectively. In odd heartbeats, a T2Prep-IR preparation module was used, with a T2Prep duration of 40 msec, and inversion time (TI) = 110 msec, while in even heartbeats only fat saturation was used. The undersampling was 3-fold for the healthy volunteers and 4-fold for the patients. 6-channel and 18-channel anterior coils were employed at 0.55T and 1.5T, respectively in combination with the spine coil. Diagnostic quality of the cardiac chambers and vessels regarding sharpness of vascular borders and robustness to artefacts was assessed and compared between the 0.55T and 1.5T acquisitions using a 1-5 Likert scale (1: non-diagnostic, 5: excellent image quality, 3: diagnostic). The signal ratio between blood and myocardium was computed in the respective intrapericardial structures.
Results:
Seven patients (mean age 30±2 years, 7 female) were scanned (Fig.1 and 2). Scan time was shorter at 1.5T, 5.2(4.7, 5.4)min vs 7.1(6.0, 8.5)min, p=0.02. Image quality scores were comparable between the two approaches (Fig.3A) for the majority of the intrapericardiac structures. Delineation of the pulmonary veins and coronary arteries was superior at 0.55T. Signal ratio (blood pool/myocardium) comparison demonstrated comparable results with both approaches for all structures, except the pulmonary and the systemic veins and the left atrium where the approach at 0.55T was superior (Fig.3B).
Conclusion:
The T2prep-IR-BOOST implemented at 0.55T, demonstrated equal or superior image quality to the respective sequence at 1.5T in a feasible scan time. The increased field homogeneity at 0.55T diminishes off-resonance artefacts at the lung-vascular interface, such as pulmonary veins. The low-rank based denoising has potentially superior performance in the 0.55T dataset of increased homogeneity, improving the delineation of systemic veins and coronary arteries [5].
Fig.2: Visual comparison between images from two patients with the proposed 3D whole-heart bright-blood iT2prep-BOOST approach at 0.55T (first row) versus 1.5T (second row). The delineation of pulmonary veins and coronary arteries is optimised at 0.55T (red arrows).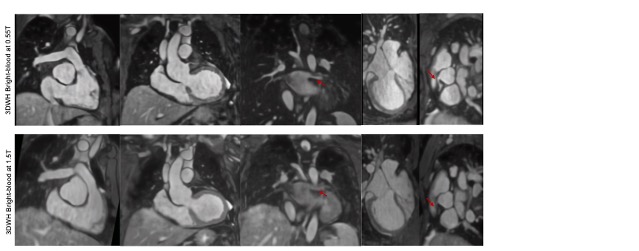
Fig. 3A: Image quality scores analysis with respect to sharpness of the vessel and robustness to artefact (1 = nondiagnostic, ≥3= diagnostic, 5 = excellent) for the proposed iT2Prep-BOOST bright- and black-blood at 1.5T vs 0.55T. 2B:SIgnal ratio comparison for the bright-blood iT2prep-BOOST approach at 0.55T versus 1.5T.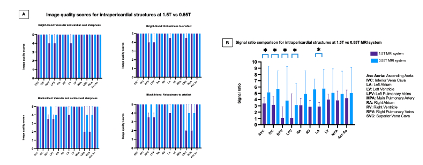
Fig.1: Visual comparison between images from two patients with the proposed 3D whole-heart iNAV-based iT2prep-BOOST approach at 0.55T (first row) versus 1.5T (second row).