Technologist Track
Cheuk Fung Yiu, BSc
Cardiac MRI Radiographer
Guy's and St. Thomas' Hospital NHS Foundation Trust, United Kingdom
Cheuk Fung Yiu, BSc
Cardiac MRI Radiographer
Guy's and St. Thomas' Hospital NHS Foundation Trust, United Kingdom

Tevfik F. Ismail, MD, PhD, BSc, FSCMR
Consultant Cardiologist/Reader (Associate Professor)
Guy's and St Thomas' Hospital/King's College London, United Kingdom
.jpeg.jpg "Filippo Bosio photo")
Filippo Bosio
Superintendent Radiographer
King's College London, United Kingdom
A 77-year-old male with known non-ischemic dilated cardiomyopathy and recurrent ventricular tachycardia (VT) with an MR conditional implantable cardioverter-defibrillator (ICD) in situ was referred for cardiovascular magnetic resonance to assess cardiac function and territory of fibrosis to guide VT ablation.
Diagnostic Techniques and Their Most Important Findings:
This study was performed on a 1.5T MRI scanner to adhere to manufacturer safety guidelines and minimise susceptibility artefacts. The ICD was programmed to 0D0 mode during the examination. Cine images were acquired using a standard steady-state free precession (SSFP) sequence with a wide bandwidth, resulting in minimal metal artefacts that did not interfere with the area of interest. Fast low-angle shot (FLASH) sequence was also attempted but the overall quality was inferior to SSFP sequences (FIG 1).
For late gadolinium enhancement (LGE) imaging, the initial protocol employed a phase-sensitive inversion recovery (PSIR) SSFP LGE sequence with breath-holding. However, due to poor image quality caused by ICD artefacts and patient fatigue from breath-holding, the imaging approach was modified by using a wideband-inversion recovery prepared LGE sequence combined with a FLASH, increased receiver bandwidth, and free-breathing motion-corrected (MOCO) techniques. The FLASH sequence applies gradient or radio frequency spoiling at the end of each short repetition time to eliminate transverse magnetisation, making it less susceptible to metal artefacts. Unlike the SSFP sequence, FLASH does not use spoiling gradients between alternating excitation pulses, resulting in a steady-state signal that exhibits a T2/T1 contrast. Recognising the patient's breathing difficulties, the radiographer adapted a free-breathing technique with 12 averages to better compensate for motion artefact and to improve signal noise (FIG 2).
Additionally, a 3D LGE sequence with wideband inversion pulses was considered an alternative to traditional 2D breath-holding LGE to provide comprehensive myocardial coverage without gaps. A respiratory navigator was set at the diaphragm level with a 3mm acceptance window to ensure consistent inversion time (TI) during the 10-minute acquisition (FIG 3).
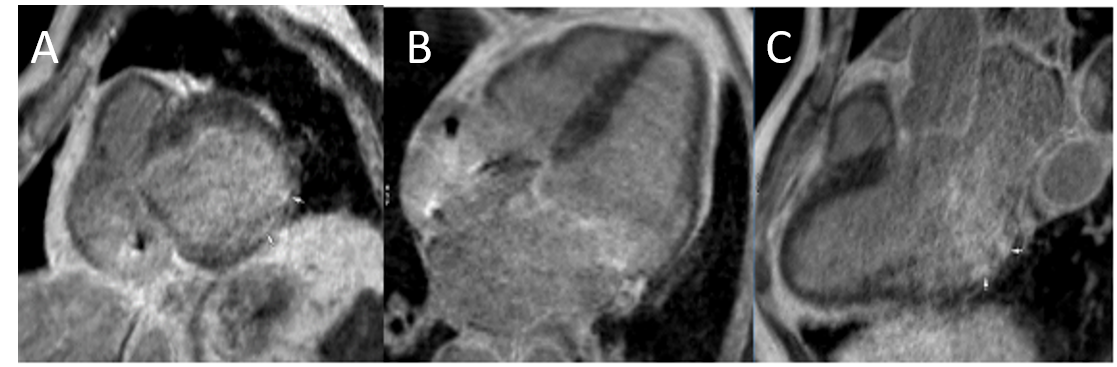
The final images revealed near-transmural infarction of the basal lateral wall, with clear LGE demonstrating myocardial fibrosis and confirming the extent of ischemic damage.
Learning Points from this Case:
The combination of wide bandwidth SSFP and FLASH with free-breathing MOCO significantly enhances the quality and diagnostic accuracy of LGE imaging in patients with ICD implants. The 3D LGE sequence provided high spatial resolution and uninterrupted coverage of the myocardium, which was crucial in assessing the extent of ischemic injury. These techniques effectively address the challenges posed by ICD artefacts and breath-holding limitations, providing high-resolution images that allow for precise assessment of myocardial fibrosis and viability. This approach is particularly beneficial for patients unable to maintain prolonged breath-holding, ensuring comprehensive and accurate CMR imaging outcomes.
FIG 1: 2 Chamber cine view in Steady State Free Precession (A) and Fast Low-Angle Shot (B) 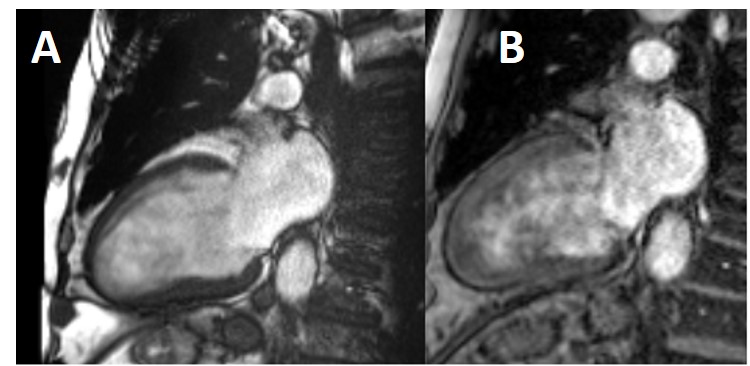
FIG 2: 4 Chamber late gadolinium enhancement in Steady State Free Precession (A). 4 Chamber (B) and short axis (C) late gadolinium enhancement in Fast Low-Angle Shot.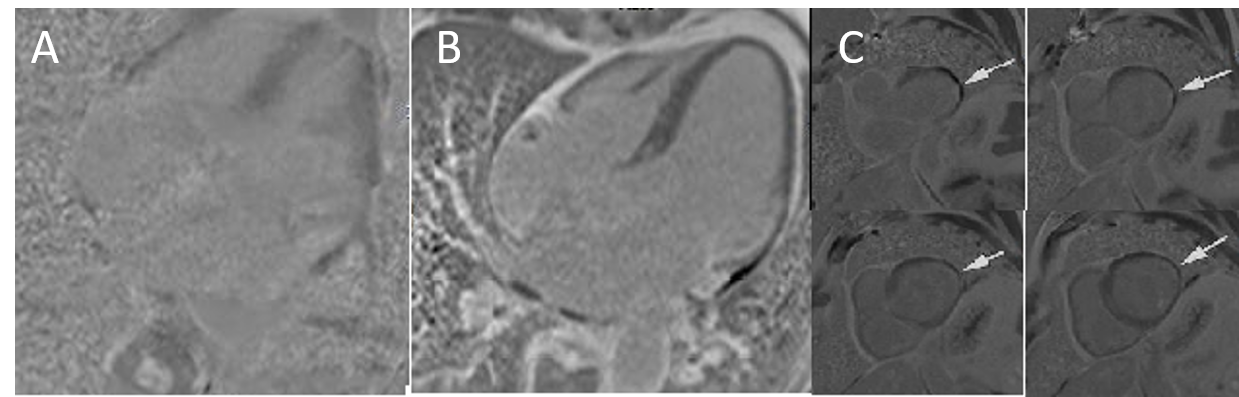
FIG 3: 3D late gadolinium enhancement with wideband inversion pulses multi-planar reconstruction in short axis (A), 4 Chamber (B) and 3 Chamber (C) views.