Oral Case
PRIYAMVADA PILLAI, MD
FELLOW PHYSICIAN
THE HEART HOSPITAL BAYLOR PLANO
PRIYAMVADA PILLAI, MD
FELLOW PHYSICIAN
THE HEART HOSPITAL BAYLOR PLANO
MODAR ALOM, MD
fellow
the heart hospital baylor plano
amro alsaid, MD
Cardiologist
Baylor Scott & White - The Heart Hospital Plano
A 39-year-old female with no significant medical history presented to the Emergency Room with intermittent substernal chest pain and palpitations. Initial hospital evaluation for acute coronary syndrome was unremarkable. During subsequent outpatient cardiology evaluation, a coronary CT angiogram revealed a 7 x 5.7 cm ovoid mass on the lateral wall of the left ventricle (LV), compressing the LV cavity. Given the concerning appearance of the LV mass, the patient was referred for further evaluation with Cardiac MRI.
Diagnostic Techniques and Their Most Important Findings:
CMR was performed on a Philips Achieva 1.5 Tesla scanner using a mass protocol. Imaging revealed a well-circumscribed 7.1 cm x 6.0 cm mass within the lateral wall of the left ventricle, causing significant compression of the LV cavity. The mass appeared hypointense compared to the myocardium on both T1-weighted and T2-weighted black blood sequences, with no signal suppression on fat saturation imaging (Figure 1). First-pass perfusion images demonstrated minimal enhancement, indicating low vascularity. However, delayed gadolinium enhancement showed marked homogeneous uptake, suggesting increased interstitial space within the mass, consistent with high fibrous content (Figure 2). These findings pointed towards a diagnosis of cardiac fibroma, a nonmalignant pathology.
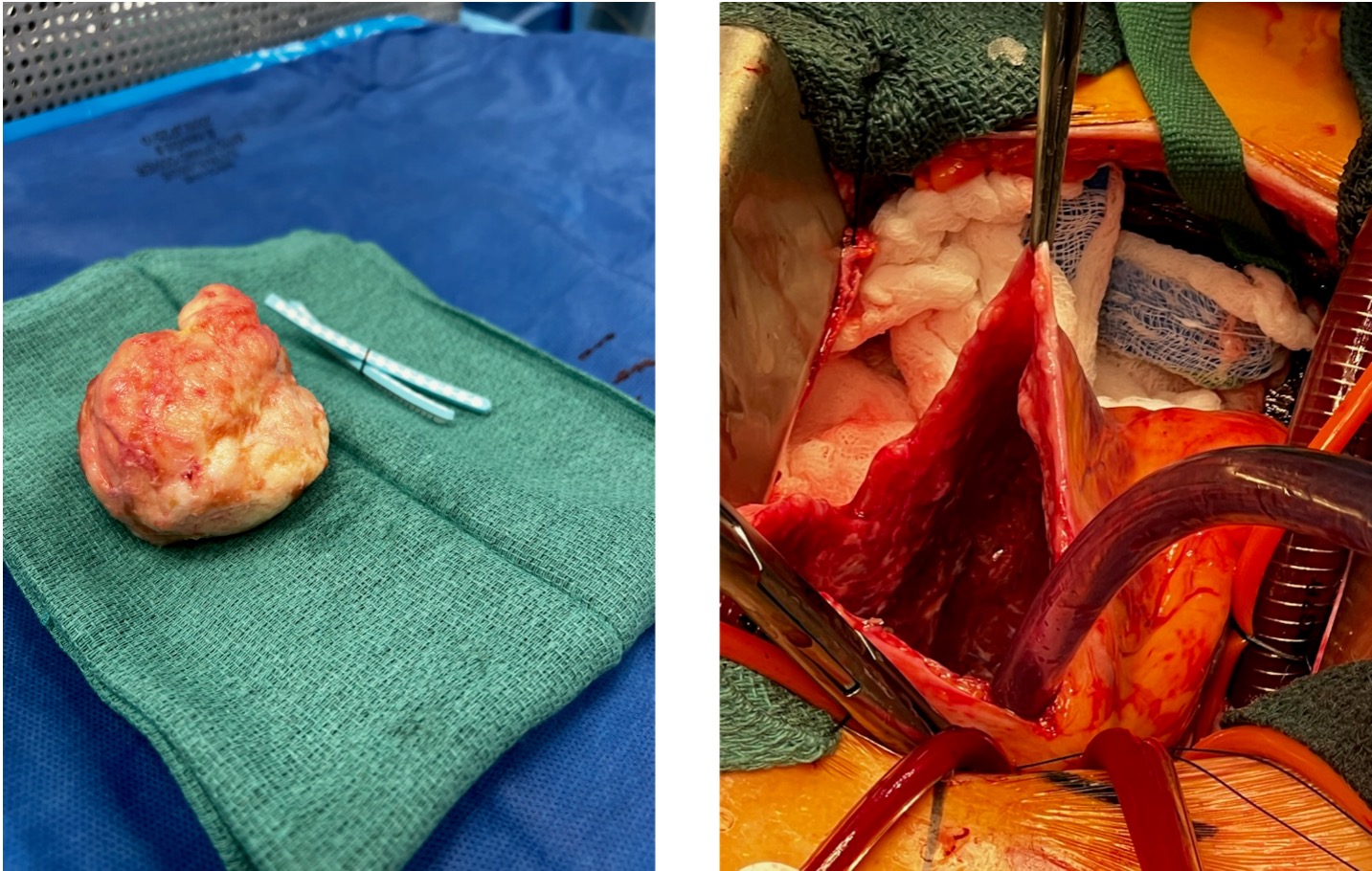
Due to the size of the mass and the patient’s symptoms, she was promptly referred for surgical resection. The excised specimen was a firm, white, encapsulated mass (Figure 3). Histopathological examination revealed eosinophilic spindle cells with thin, ovoid, compressed nuclei and no evidence of malignancy, confirming the diagnosis of cardiac fibroma.
Learning Points from this Case:
Cardiac fibromas are a rare clinical entity in adults, with the majority of patients being asymptomatic. However, unlike other benign tumors, large cardiac fibromas carry a significant risk of ventricular arrhythmias and sudden cardiac death, making early detection crucial for preventing serious cardiac complications. This case underscores the importance of recognizing key Cardiac MRI findings to establish a definitive clinical diagnosis. By doing so, unnecessary additional testing can be minimized, and definitive therapy, such as surgical intervention, can be expedited to improve patient outcomes.
. a. T1 weighted black blood axial image at end diastole with hypointense mass in LV lateral wall as compared to myocardium. b . T2 weighted black blood image and T2 weighted fat saturation image showing hypointese LV mass as compared to myocardium. C. Cine image with hypointense homogenous mass as compared to myocardium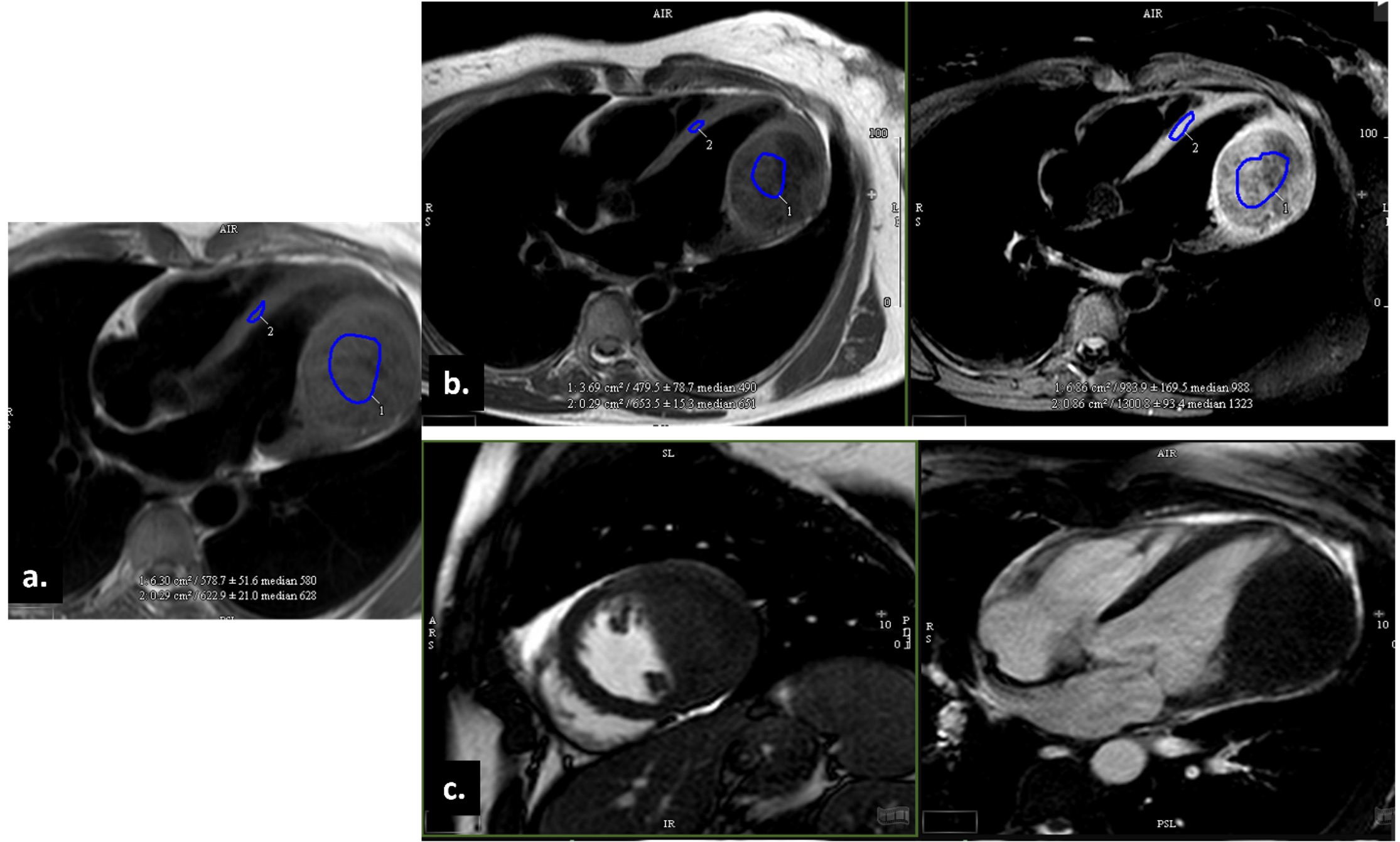
a. First pass perfusion image with minimal contrast uptake within the mass as shown with the white arrow. b. Delayed post gadolinium enhancement with increased homogenous uptake suggesting increased interstitial space within the mass, consistent with high fibrous content 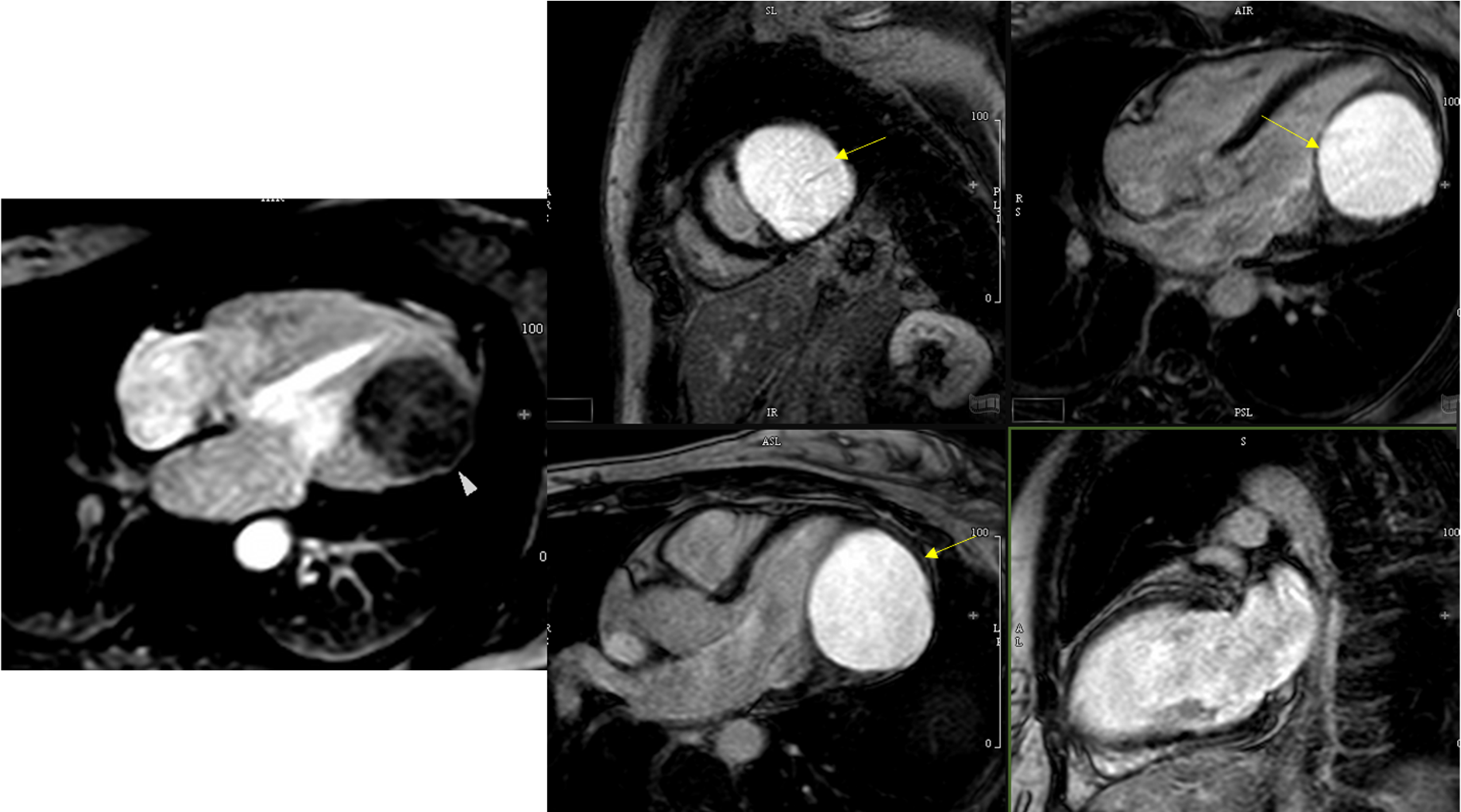
Gross pathology of excised cardiac mass.