Description of Clinical Presentation: A 19-year-old male with past medical history of Kawasaki disease previously treated with IVIG presented with several hours of chest pain that radiated to the jaw. An EKG showed diffuse nonspecific ST changes without reciprocal changes, and the initial high sensitivity troponin was 19,734 ng/L. He was taken for urgent coronary angiography which demonstrated occlusion of an obtuse marginal branch disproportional to the degree of troponin elevation, therefore consistent with myocardial infarction with non-obstructive coronary artery disease (MINOCA). Given the history of Kawasaki disease and inconclusive angiography, the decision was made to pursue CMR to further differentiate between coronary artery abnormalities or myocardial disease.
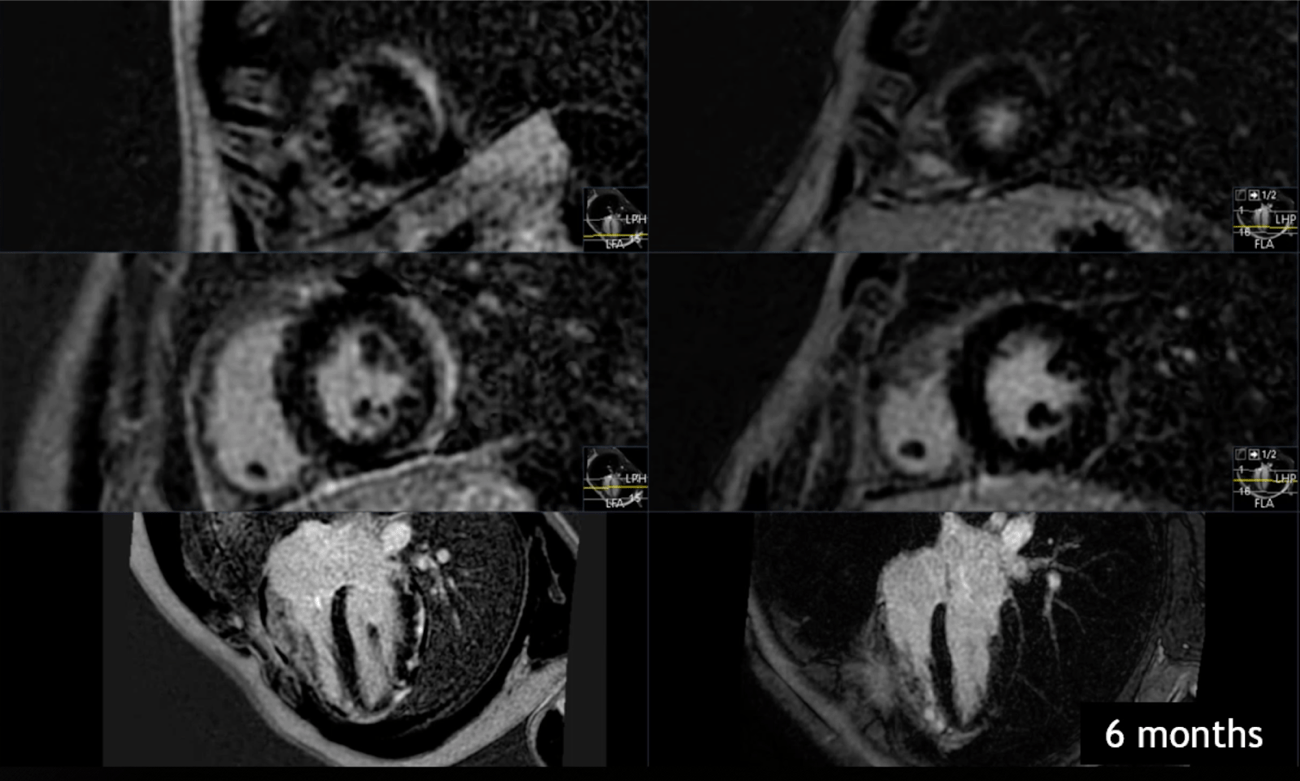
Diagnostic Techniques and Their Most Important Findings: CMR native myocardial T1 mapping (MOLLI) was significant for prolonged relaxation of the left ventricular lateral wall extending from base to apical region (Figure 1). T2 dark-blood imaging had focal areas of increased signal which correlated with areas of T1 mapping, suggestive of myocardial edema in the epicardium and mid myocardium (Figure 2). There was also delayed myocardial hyperenhancement of the mid-myocardium and subepicardium involving the basal inferolateral and anterolateral walls as well as pericardial delayed hyperenhancement along the apical anterior and lateral walls (Figure 3). These findings were all consistent with the diagnosis of myopericarditis, therefore an anti-inflammatory regimen of aspirin and colchicine therapy were initiated. Follow up CMR at 6 months after completion therapy showed normalization of T1, T2, and delayed enhancement findings (serial imaging shown, Figures 1-3).
Learning Points from this Case: The spectrum of cardiovascular disease in Kawasaki Disease extends beyond early childhood and beyond coronary artery disease. Myopericarditis is postulated to be far more common than coronary artery disease and is under-appreciated in children and adults.CMR was essential for the appropriate diagnosis of myopericarditis in this patient with history of Kawasaki disease found to have MINOCA, ultimately leading to appropriate treatment and resolution of CMR abnormalities. CMR can be used in other cases in which coronary angiography is inconclusive or incongruent with clinical presentation.
Figure 1. T1 mapping at time of presentation (left) compared to 6 month follow-up imaging (right). Figure 2. T2 mapping (left) with correlated T1 mapping (right). Figure 3. Delayed enhancement imaging at time of presentation (left) compared to 6 month follow-up imaging.

.png)
.png)