Oral Case
Maya Kailas, MD
Fellow
Mount Sinai

Kenan Stern, MD
Associate Professor of Pediatrics and Radiology
Director, Non-invasive Imaging
Director, Pediatric Adanced Cardiac Imaging Fellowship
Icahn School of Medicine at Mount Sinai

Nadine Choueiter, MD
Director of Pediatric cardiac non invasive imaging
Kravis Children's Hospital at Mount Sinai
David Barris, MD
Assistant Professor of Pediatric Cardiology
Icahn School of Medicine at Mount Sinai, Mount Sinai Kravis Children’s Hospital
Neha Bansal, MD
Associate Professor
Mount Sinai
An 18 year old female with a history of asthma and uveitis developed and thigh mass and a groin mass. Biopsy and dermatopathology revealed the diagnosis of Rosai Dorfman disease. Given that the diagnosis is associated with systemic and cardiovascular involvement, she received a multi-modality imaging workup and was referred to cardiology.
Diagnostic Techniques and Their Most Important Findings:
Initially a PET scan was done to evaluate the extent of the disease. Diffuse uptake was seen around a thoracic aorta, bilateral thighs, mesentery, left ovary, and hilar lymph nodes. Given aortic involvement, as well as the known small risk of cardiac masses in Rosai Dorfman, she underwent further cardiac imaging.
Echo was done as part of a standard cardiac work-up. No masses or structural defects were identified.
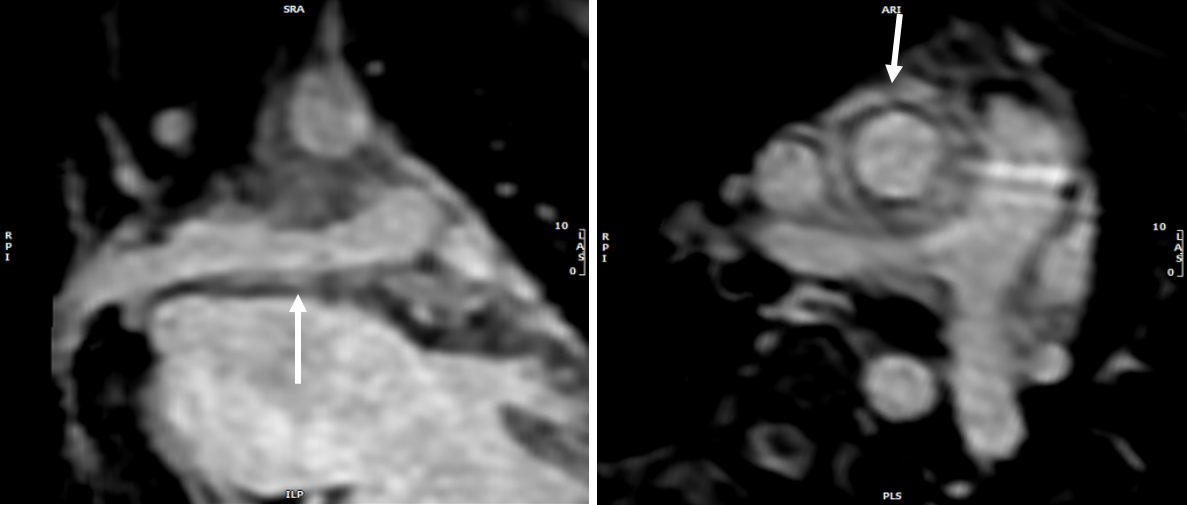
Cardiac MRI was ultimately done to further characterize the aortitis found on PET scan. A 4.2cm x 1.7cm oblong mass was found in the anterior RV wall without impairment in RV function. There was also tissue encasing the aorta extending from the level of the aortic root to the base of the head and neck vessels. This tissue also encased the right pulmonary artery and partially the main pulmonary artery. Lastly, there was additional tissue encasing the thoracic descending aorta extending from level of the pulmonary veins to the level of the renal arteries.
Compared to the myocardium, the cardiac mass in the RV wall was isointense on Cine SSFP, T1, and T2 images. It did not suppress on T1 fat saturation. It did not enhance on first pass perfusion. It exhibited late gadolinium enhancement. Given that these imaging findings are consistent with Rosai Dorfman disease, as well the non-cardiac pathologic diagnosis, these cardiac lesions were presumed to be further involvement of Rosai Dorfman.
Learning Points from this Case:
Rosai Dorfman is a disease of non-malignant histiocyte proliferation that is thought to be due to an exaggerated immune response to a viral trigger versus having a genetic cause. It usually presents as painless cervical lymphadenopathy, but has extra-nodal involvement in 40% of cases. Cardiac involvement is rare, but occurs in 0.1-0.2% of cases. When present, it generally occurs as an intra-cardiac or pericardial mass, or it can occur as vessel wall thickening giving a vasculitis-like picture. This case presented as both.
This case demonstrated how cardiac MRI can be used to diagnose and follow non-cardiac diseases. Characterizing the mass using different MRI sequences allowed for a non-invasive diagnosis of this patient’s cardiac mass.
She was eventually started on targeted therapy, Cobimetinib, which is a MEK inhibitor. Her cardiac mass and extra-cardiac lesions were followed on serial PET scans, and within 6 months they all demonstrated near-resolution.
Figure 1: Tissue Characterization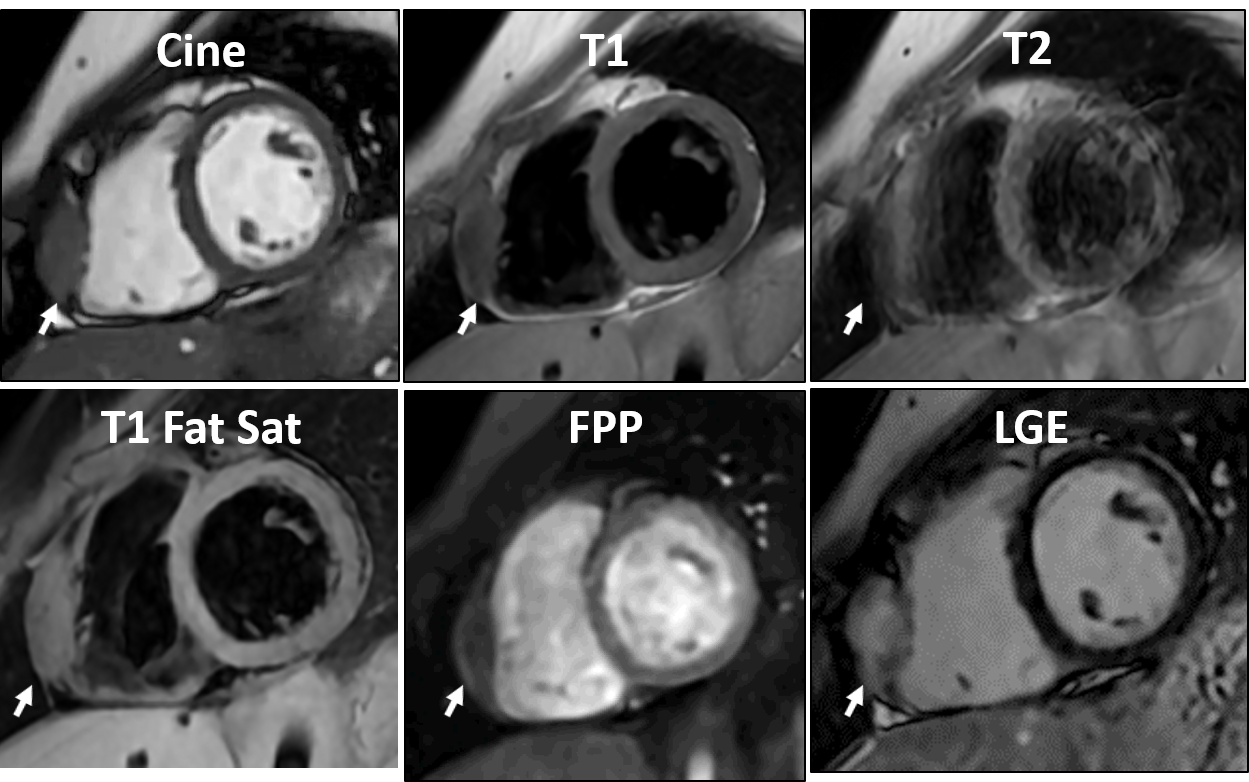
Figure 2: 3D SSFP (Sagittal)
Figure 3: 3D SSFP (Coronal and Axial)