Science Sessions
Ohta Yasutoshi, MD, PhD
Head physician
National Cerebral and Cardiovascular Center, Japan
Ohta Yasutoshi, MD, PhD
Head physician
National Cerebral and Cardiovascular Center, Japan
Tomoro Morikawa, MD
Physician
National Cerebral and Cardiovascular Center, Japan
Tatsuya Nishii, MD, PhD
Head Physician
National Cerebral and Cardiovascular Center, Japan
Morita Yoshiaki, MD, PhD
Head Physician
National Cerebral and Cardiovascular Center, Japan
Hiroki Horinouchi, MD, PhD
Physician
National Cerebral and Cardiovascular Center, Japan
Akiyuki Kotoku, MD, PhD
Physician
National Cerebral and Cariovascular Center, Japan
Midori Fukuyama, MD
Physician
National Cerebral and Cardiovascular Center, Japan
Emi Tateishi, MD, PhD
Physician
National Cerebral and Caridovascular Center, Japan
Tetsuya Fukuda, MD, PhD
Director
National Cerebral and Cardiovascular Center, Japan
The Inversion Recovery Late Gadolinium Enhancement (IR-LGE) imaging method provides high contrast for depicting myocardial lesions. Still, inappropriate inversion time (TI) settings can lead to incomplete examinations, burdening the examiner. Although it has been reported that synthetic LGE can be created from T1 mapping, it is difficult to image simultaneously and compare images. Using dynamic T1 mapping for pharmacokinetic analysis makes it possible to create T1 maps from concentrations at any given time, allowing image evaluation with precisely matched imaging times. This study aims to investigate whether synthetic IR-LGE created from T1 maps adjusted to the post-imaging time of actual IR-LGE scan using pharmacokinetic analysis can achieve image quality, contrast, and lesion detection equivalent to actual IR-LGE.
Methods:
50 participants who had planned CMR for myocardial evaluation (61 years, IQR 48,73) were included in this study. Actual LGE imaging (aLGE) was performed 10 minutes after contrast medium injection following TI-scout image acquisition for all participants using the inversion recovery method. Additionally, contrast agent concentrations at each time point were calculated from sequentially acquired T1 maps, and the T1 map 10 minutes after contrast administration was computed using a myocardial contrast agent concentration pharmacokinetic analysis model. Synthetic inversion recovery LGE images (sLGE) were created with TI ranging from 220 ms to 400 ms based on pharmacokinetics-derived T1 maps. Heart rate during scan was also reflected in the sLGE signal values. The null point TI of the myocardium was recorded in the Look-Locker TI-scout image and sLGE. Using sLGE images with the same TI as for aLGE imaging, sLGE and aLGE images were evaluated for image quality (5 points: 1; non-diagnostic, 5; excellent), pattern (endocardial, epicardial, mesial, ischaemic, transmural, none) and contrast ratio between LGE lesion and remote myocardium.
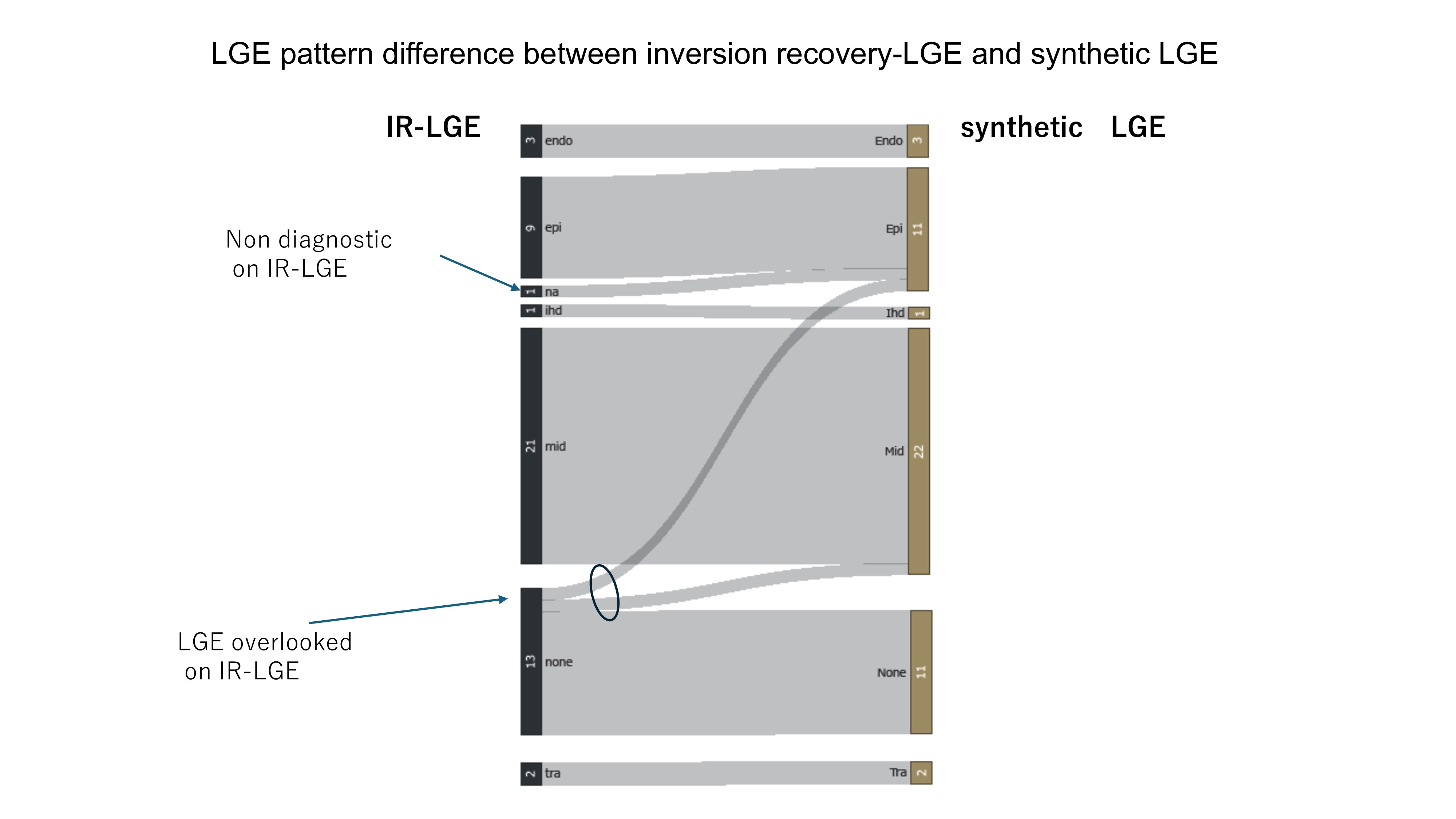
Results: The TIs of the null myocardium point were 320±25msec with TI-scout and 316±22msec with sLGE (p=0.01). The image quality score was higher for sLGE compared to aLGE (4.7 vs. 4.3, p=0.03). The enhancement patterns were classified for aLGE and sLGE as follows: endocardium 3 vs. 3, epicardium 9 vs. 11, mid 22, ischemic 1 vs. 1, transmural 2 vs. 2, none 13 vs. 11, respectively. One non-diagnostic case was identified in aLGE. There was one case each where epi and mid were determined in sLGE but classified as none in aLGE. The contrast ratio of LGE was higher for sLGE compared to aLGE (0.70 vs. 0.58, p< 0.01).
Conclusion: Synthetic LGE created from T1 maps aligned with LGE imaging time using pharmacokinetic analysis can be used for myocardial lesion evaluation equivalent to IR-LGE.
46-years-old man, with dilated cardiomyopathy The left panel shows conventional inversion-recovery LGE (TI=310 msec), the right panel shows synthetic LGE from a pharmacokinetics-derived T1 map (TI=310 msec) A mid-wall linear high-intensity lesion is shown in both images.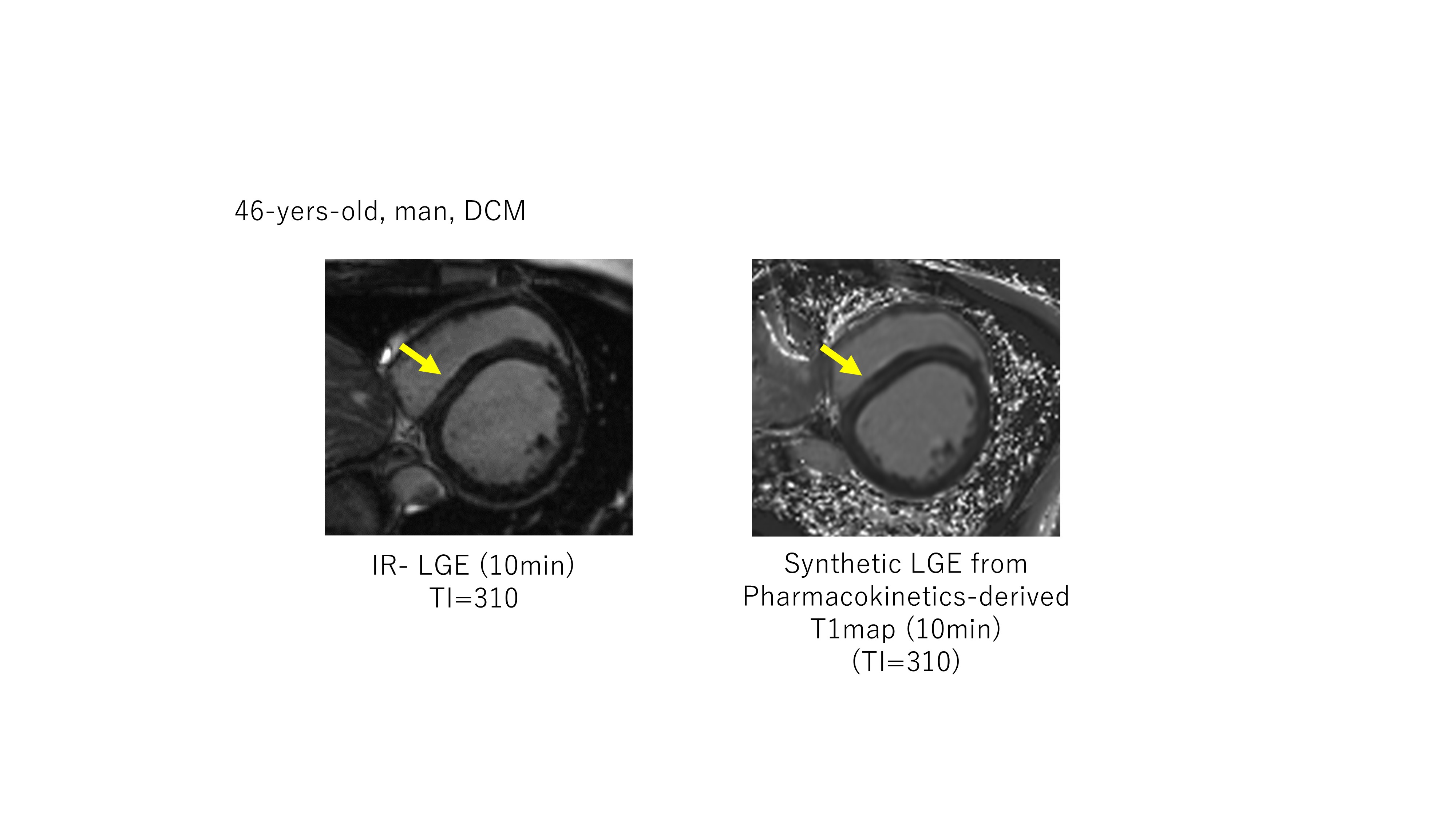
LGE pattern difference between IR-LGE and synthetic LGE