Rapid Fire Abstracts
Andres F. Moreno Rojas, MD
Post Doctoral Clinical Fellow
Stanford University
Andres F. Moreno Rojas, MD
Post Doctoral Clinical Fellow
Stanford University
Meaghan J. Beattie, MD
Clinical Assistant Professor
Stanford University

Sujatha Buddhe, MD
Professor
Stanford University
Anitra W. Romfh, MD
Clinical Associate Professor
Stanford University
Ali Syed
Clinical Assistant Professor
Stanford University

Shiraz A. Maskatia, MD
Clinical Professor
Stanford University School of Medicine
In single-ventricle patients with Fontan palliation, percent collateral flow (%CF) is frequently assessed by cardiac MRI (CMR), using either systemic (%CFs) or pulmonary (%CFp) flow, as it affects early and long-term outcomes, ventricular size, and function. CPET has been demonstrated to have also prognostic value in Fontan patients, as lower VO2 has been associated with increased morbidity and mortality. We investigated the associations between %CF as measured on 4-dimensional phase contrast (4DF) CMR and measures of exercise capacity.
Methods:
We performed a single-center, retrospective review of patients status post-Fontan procedure who underwent ferumoxytol-enhanced 4DF CMR from January 2022 to December 2023, with cardiopulmonary exercise test (CPET) performed within 1 year. %CF was measured as follows: %CFs = (systemic arterial – systemic venous flow)/systemic arterial flow, %CFp = (pulmonary vein – pulmonary artery flow)/pulmonary vein flow. Other CMR measurements collected include indexed ventricular end-diastolic (iEDV) and end-systolic (iESV) volumes and ejection fraction. CPET performance was categorized as normal, low normal, mild, moderate or severe. Descriptive data are presented as mean (SD). Pearson correlation was used to compare continuous variables. ANOVA and t-test were used to compare categorical and continuous variables. Analyses were performed using R Statistical Software (v4.4.1).
Results:
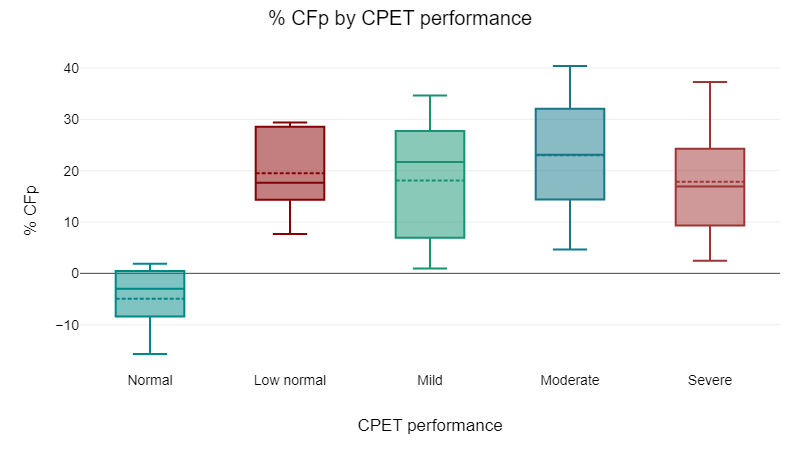
Forty-five patients met inclusion criteria, and 11 (24.4%) were excluded due to CPET with submaximal effort. The demographics and summary of CMR and CPET data is included in Table 1. The calculated %CFs was higher (M = 17.19, SD = 16.52) than the %CFp (M = 16.64, SD = 13.55) but this difference was not statistically significant (t = 0.36, p = .724). There was a very high and significant correlation between %CFs and %CFp (r = 0.85, p = < .001). There was moderate and significant correlation between %CFp and VO2 max/kg while there was only a trend towards a mild correlation between %CFs and VO2 max/kg (Table 2). The percentage difference of flow between the right and left pulmonary veins had also a moderate and significant correlation with VO2 max/kg and % predicted VO2 max (Table 2). %CFp was different based on CPET performance category (F = 4.37, p = .007), with a significantly different pairwise comparison between the group with “normal exercise capacity” and any of the other groups (p-value < 0.05) (Figure 1). There was no significant difference in any other CMR measurement and CPET performance category, including: ejection fraction, atrioventricular valve regurgitation, aortic regurgitation, EDV, and ventricular morphology.
Conclusion:
In this pilot cohort of adolescent and young adult Fontan patients, increased %CFp was associated with abnormal exercise capacity. Although %CFs and %CFp correlated well, %CFp appeared to be more closely associated with exercise capacity.
Figure 1 Comparison of %CFp by CPET performance