Oral Abstract
Briella K. Egberts, BBiomed, BMedSci (hons), PhD Candidate
PhD Candidate
Flinders University, Australia
Rajiv Ananthakrishna, MD
Consultant Cardiologist
Flinders Medical Centre, Australia
Ranjit J. Shah, MD, PhD
Cardiologist
Flinders University, Australia
Joseph Justin Regalado, MD
CMR Fellow
Flinders Medical Centre, Australia
Antony Chun Fai So, MD
Fellow/ PhD candidate
Flinders Medical Centre, Australia
Alison Sutton, RT
Radiographer
Flinders Medical Centre, Australia
Leah McWilliams, RN
Nurse Practitioner
Royal Adelaide Hospital, Australia
Jennifer Walker, MD, PhD
Consultant
Royal Adelaide Hospital, Australia
Sivabaskari Pasupathy, PhD
Post Doc Fellow
Flinders University, Australia
Susanna Proudman, PhD
Royal Adelaide Hospital, Australia

Joseph Selvanayagam, MBBS DPhil
Director
Flinders University, Australia
Myocardial fibrosis is the pathological feature of primary heart involvement in systemic sclerosis (SSc-pHI) and is thought to result from repeated focal ischemia due to microvasculopathy. Right ventricular (RV) dysfunction is common is SSc and typically arises from increased pulmonary arterial load due to pulmonary artery hypertension (PAH). Oxygen sensitive cardiac magnetic resonance imaging (OS-CMR) directly visualises in-vivo myocardial deoxygenation and subsequent ischemia. We aimed to detect RV myocardial ischemia in SSc to better characterise subclinical RV microvasculopathy using RV-targeted OS-CMR imaging.
Methods: SSc patients without known cardiac disease, patients with stable PAH of any aetiology and normal healthy volunteers (NV) were prospective enrolled. All patients underwent a 3T CMR. The primary outcome was change in inferior RV OS-CMR signal intensity (SI).
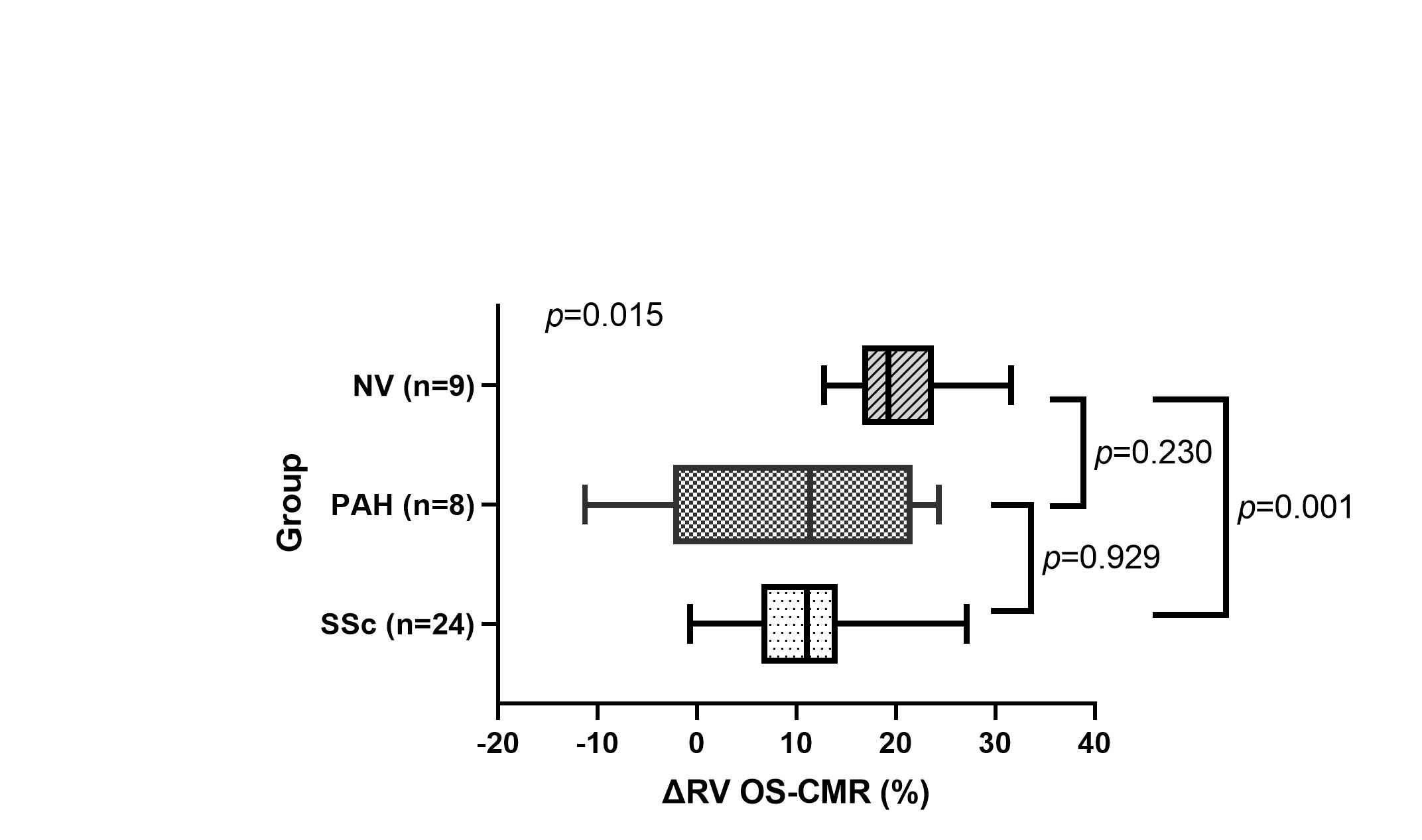
Results: A total of 46 patients (26-SSc, 10-PAH, 10-NV) were enrolled. The RV OS-CMR SI was significantly lower in the SSc group compared to the NV group (10.56±9.32 vs 20.80±5.94, p=0.001). There was no significant difference between the PAH and SSc groups (9.02±14.40 vs 10.56±9.32, p=0.929), indicating a similar degree of RV ischemia in established PAH patients and SSc patients.
Conclusion: SSc patients had evidence of RV Ischemia relative to NV. These findings imply that RV ischemia occurs in patients with SSc as a primary feature of the disease representing early ischemic and/or fibrosis in SSc patients. Our findings may have screening and/or therapeutic implications.
Figure 1 Distribution of mean ∆RV OS-CMR between SSc, PAH and NV groups SSc= systemic sclerosis, PAH= pulmonary artery hypertension, NV= normal volunteer, RV= right ventricle, OS-CMR= oxygen sensitive cardiovascular magnetic resonance