P/CHD
Snigdha Bhatia, MD
Fellow
Children's Healthcare of Atlanta
Snigdha Bhatia, MD
Fellow
Children's Healthcare of Atlanta

Sassan Hashemi, MD
Research Scientist
Children's Healthcare of Atlanta
William A. McEachern, MD
Assistant Professor of Pediatrics
Emory University/Children's Healthcare of Atlanta

Hunter C. Wilson, MD
Assistant Professor of Pediatrics
Emory University

Timothy Slesnick, MD
Pediatric Cardiologist
Children's Healthcare of Atlanta
A 13-year-old healthy female suffered traumatic dissection of her aorta in a motor vehicle collision. She developed a pseudoaneurysm on the undersurface of the aortic arch and underwent a thoracic endovascular aortic repair (TEVAR) to address the pseudoaneurysm with a Cook Zenith Alpha 18-105 covered self-expanding endograft. She tolerated the procedure well with no post-procedure complications. On serial echocardiographic evaluations, mild flow acceleration was noted across the stented region. In the presence of these findings and persistent hypertension, she underwent CMR to delineate flow dynamics across the stented aortic arch.
Diagnostic Techniques and Their Most Important Findings:
CMR was performed on a 1.5T magnet, 12 months after the procedure and showed mild narrowing at the distal end of the endograft with a peak velocity of 3.1 m/s. The aortic measurements were normal, with the narrowest distal endograft dimension measuring 12 x 12 mm and the aorta distal to the endograft measuring 18 x 18 mm. The ascending aorta was mildly dilated (31 x 29 mm, z score +3.2). Analysis of the 4-dimensional phase contrast imaging demonstrated a normal right-handed helical pattern in the ascending aorta and a small recirculation vortex beginning at the inferior edge of the endograft consistent with mild stenosis. The peak velocity by four-dimensional phase contrast imaging was 3.1 m/s similar to the 2D flow measurement. Interestingly, although there was a susceptibility artifact from the endograft, it was limited to the metallic struts of the graft, allowing for a comprehensive assessment of the aortic arch.
Learning Points from this Case:
This case illustrates the use of CMR and four-dimensional phase contrast imaging for the assessment of flow across an aortic endograft placed in a patient who had experienced aortic dissection. A Cook Zenith Alpha covered self-expanding endograft is MRI conditional, and despite mild susceptibility artifact, CMR was able to provide unique information about the flow characteristics throughout the endograft. Mild flow convergence and vortex formation at the distal edge of the endograft were noted, which merits surveillance. A reassuring right-handed helical pattern, with mild stenosis on 2D and 4D measurements, supported routine surveillance of the endograft. On the most recent follow-up 7 years later, the patient remains asymptomatic, with mild distal stenosis and mild hypertension controlled with metoprolol.
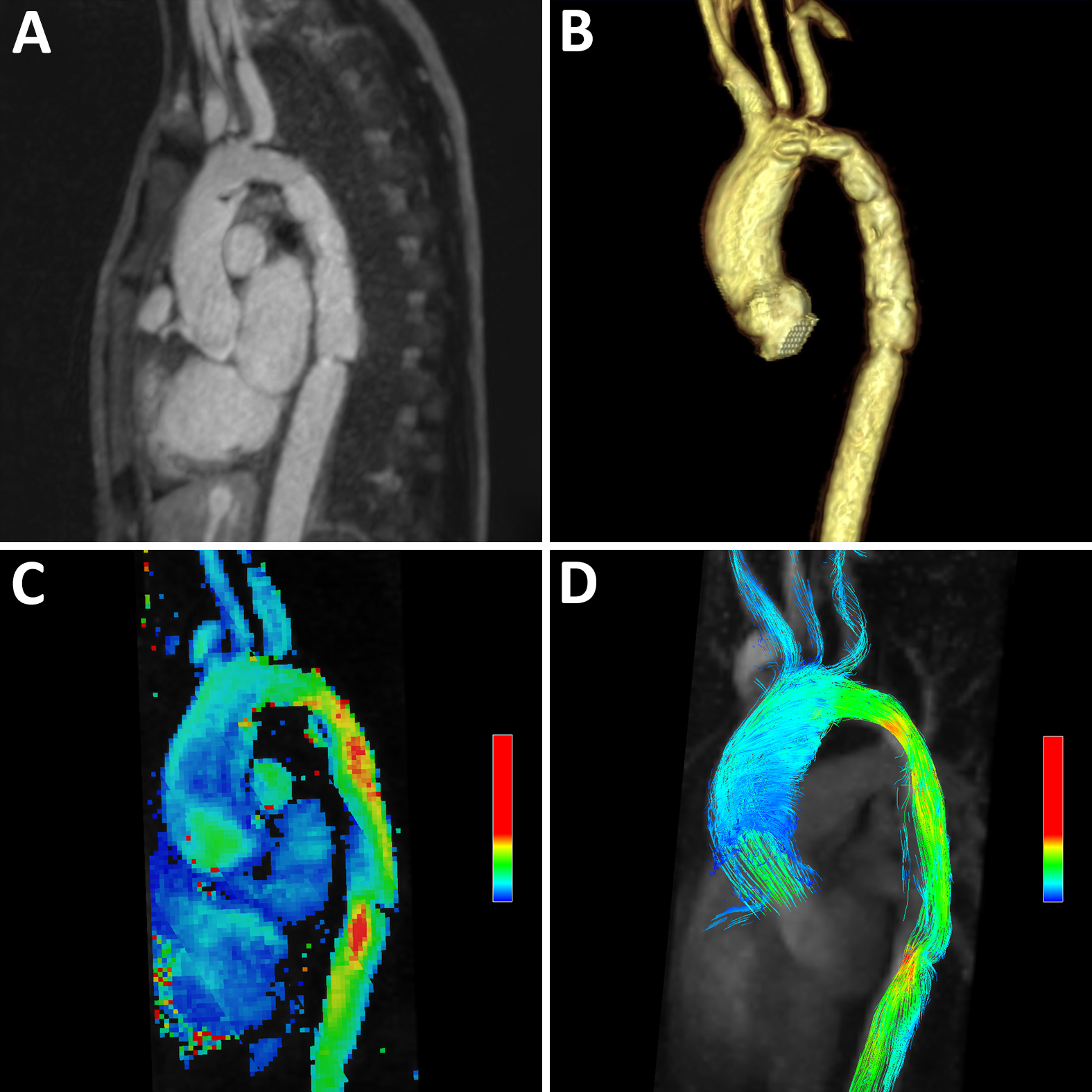
Panel A: Sagittal slice from contrast-enhanced MRA showing the endograft extending from transverse aortic arch to mid-descending thoracic aorta with minimal artifact, Panel B: Three-dimensional reconstruction of the same dataset showing mild narrowing at the distal end of the graft, Panel C: Inplane heat map of the aortic arch showing significant flow acceleration at the distal end of the graft, Panel D: 4D velocity trace showing normal right helical flow pattern in the ascending aorta and significant eccentric flow convergence in the descending aorta beginning at the origin of the endograft.