Rapid Fire Abstracts
Hideharu Oka, MD, PhD
Assistant professor
Asahikawa Medical University, Japan
Hideharu Oka, MD, PhD
Assistant professor
Asahikawa Medical University, Japan
Yuki Shibagaki, MD
Clinical Fellow
Nayoro City General Hospital, Japan
Yuki Sasaki, MD
Clinical Fellow
Asahikawa Medical University, Japan
Rina Imanishi, MD
Clinical Fellow
Asahikawa Medical University, Japan
Kouichi Nakau, MD
Senior Lecturer
Asahikawa Medical University, Japan
The left and right ventricles of the heart interact with each other by sharing an epicardium. This is called “ventricular interaction”. This condition is recognized after surgery for congenital heart disease such as tetralogy of Fallot. Right ventricular enlargement caused by pulmonary valve regurgitation, one of the postoperative complications, not only reduces right heart function but also affects left heart function. However, the pathogenesis of ventricular interaction is difficult to evaluate. The 4D flow MRI enables quantitative evaluation of intraventricular blood flow and may be applied to the assessment of ventricular interaction. This study aimed to evaluate the ventricular interaction based on intraventricular kinetic energy dynamics.
Methods:
Thirteen post-operative congenital heart disease patients (12-37 years old, 11 with tetralogy of Fallot, 1 with double-outlet right ventricle, 1 with pulmonary atresia with intact ventricular septum), 1 with idiopathic pulmonary arterial hypertension (23 years old) and 7 healthy subjects (13-26 years old) underwent 4D flow MRI. Cardiac MRI was a 3.0 Tesla whole-body imager (MAGNETOM Vida 3 T; Siemens Healthcare). Scan parameters included: acceleration method, GRAPPA 3; field of view, 340×340 mm; flip angle, 8°; temporal resolution, 41 ms; a retrospective electrocardiogram triggered. Acquired voxel size was 2.5×2.5×2.5 mm3, with velocity encoding 150 cm/s, segment 2, and 30 frames/cycle. A workstation (cvi42, Circle) was used for the analysis. The kinetic energy was calculated by dividing by the cardiac output of each ventricle (KE/CO, μJ/L/min), and the ventricular interaction was evaluated.
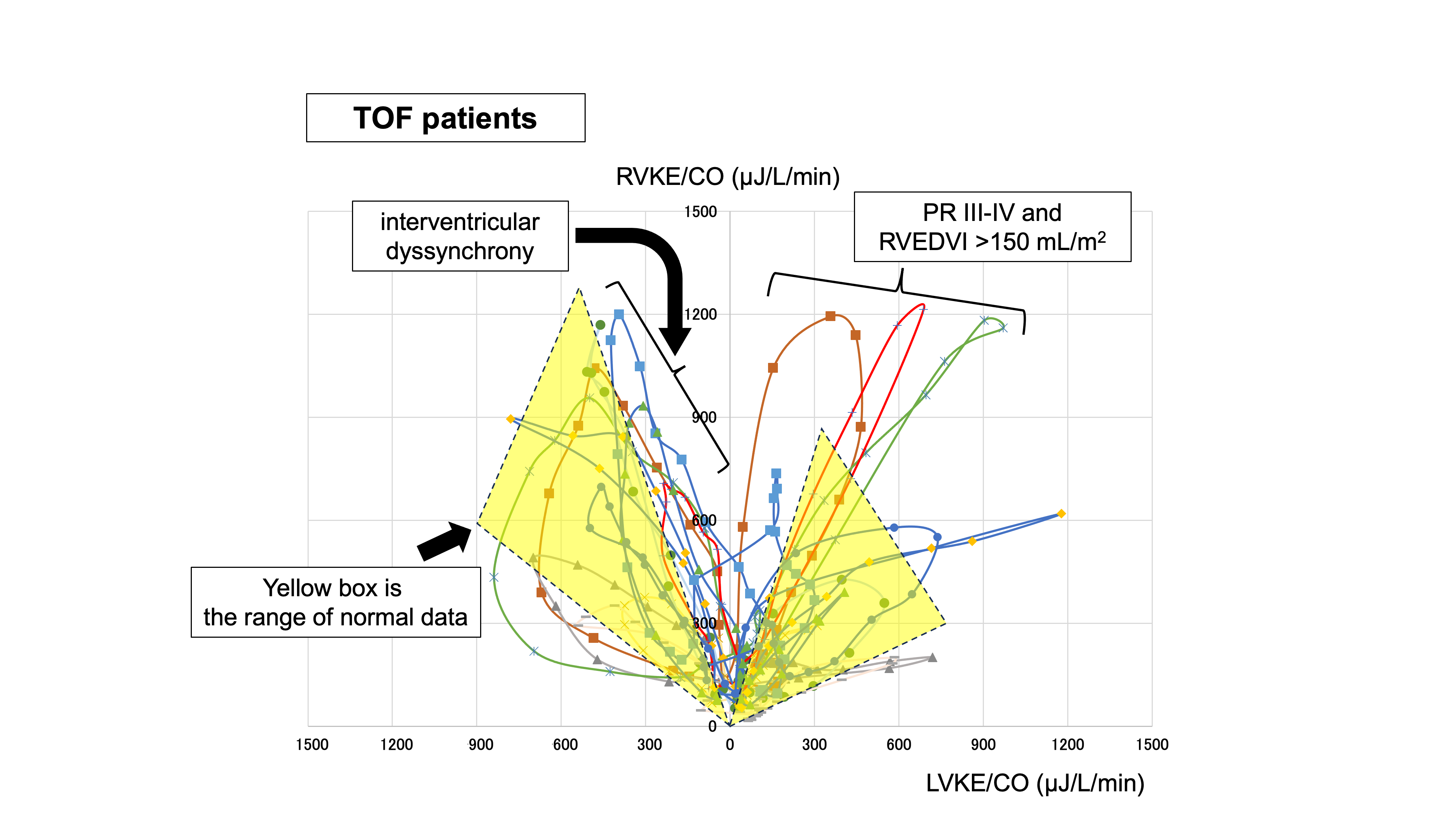
Results: The kinetic energy patterns of normal subjects were as follows: the peak of LVKE/CO was about 900 μJ/L/min and RVKE/CO was about 1200 μJ/L/min during systole, and the peak of LVKE/CO was about 600 μJ/L/min and RVKE/CO was about 800μJ/L/min during diastole, showing a constant trend. In the patient group, 5 patients showed waveforms close to the normal pattern (PR I-III degree, RVEDVI 59-130 mL/m2). On the other hand, three patients with PR III-IV degrees and RVEDVI >150 mL/m2 showed high diastolic RVKE/CO values of about 1200 μJ/L/min. In addition, 5 other patients were observed to have a slow decline in systolic RVKE/CO. This may represent interventricular dyssynchrony due to the time difference between left ventricular relaxation and right ventricular contraction. We think that patients with this waveform should be carefully monitored for left ventricular dysfunction.
Conclusion:
The use of intraventricular kinetic energy in the evaluation of ventricular interaction has the potential to visually represent not only right ventricular enlargement but also its effect on the left ventricle.
Normal ventricular interacution curve by kinetic energy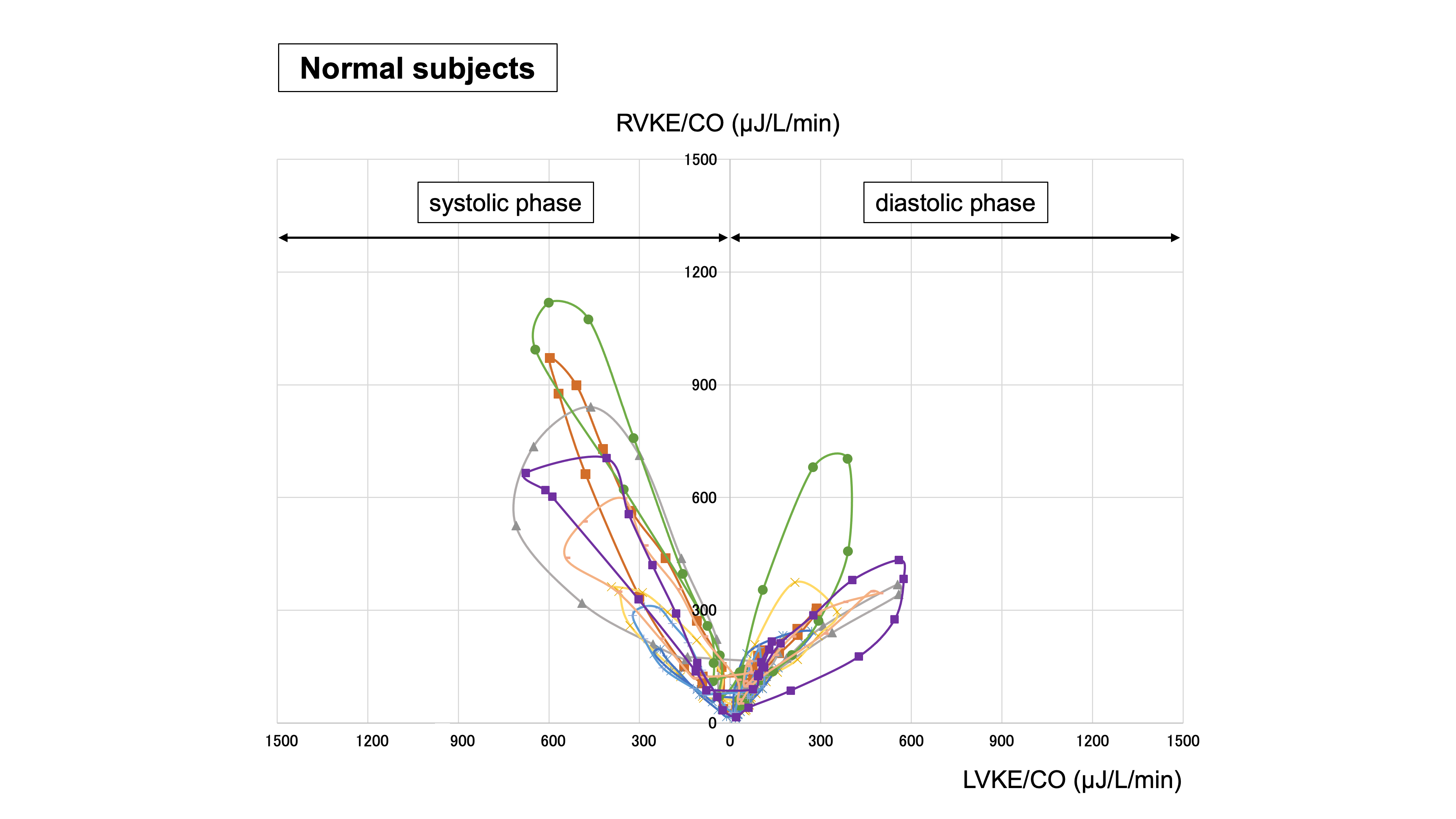
TOF patients ventricular interacution curve by kinetic energy