
Rapid Fire Abstracts

David C. Wendell, PhD
Senior Research Associate
Duke University Medical Center
David C. Wendell, PhD
Senior Research Associate
Duke University Medical Center
Han Kim, MD
Associate Professor of Medicine
Duke University Medical Center
Elizabeth Jenista, PhD
Research Scholar
Duke Cardiovascular Magnetic Resonance Center

Clerio F. Azevedo, MD, PhD
Cardiologist
Minneapolis Heart Institute at Abbott Northwestern Hospital
Fawaz Alenezi, MD
Assistant Professor of Medicine
Duke University Medical Center
Céleste Chevalier, MD
Postdoctoral fellow
Duke University Medical Center
Stephen Darty, BSc
Cardiovascular MRI technologist
Duke Cardiovascular Magnetic Resonance Center
George Gamoneda, RT
MR Technologist
Duke University Hospital
Nestor Mena, RT
MR Technologist
Duke University Hospital
Wolfgang Rehwald, PhD
Staff Scientist
Siemens Healthineers
Enn-Ling Chen, PhD
Research Professor
Duke Cardiovascular Magnetic Resonance Center
Michele Parker, MSc
Statistician / Business Manager
Duke Cardiovascular Magnetic Resonance Center
Raymond J. Kim, MD
Professor of Medicine and Radiology
Duke University Medical Center
.jpg)
.jpg)
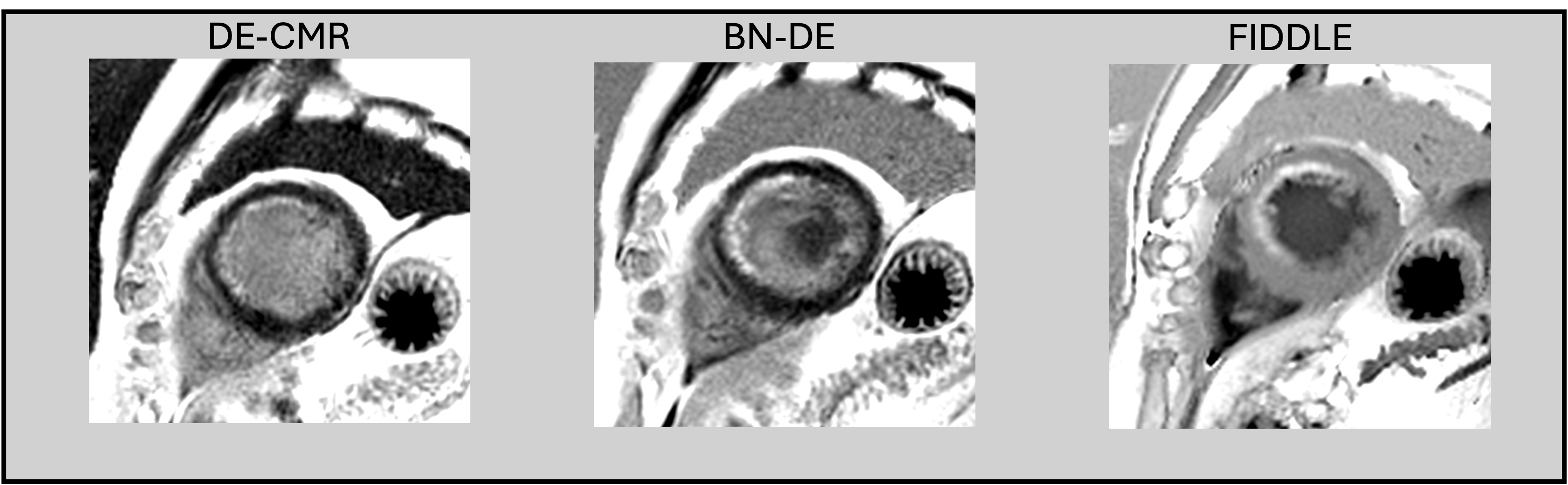
FIDDLE demonstrated better diagnostic performance than BN-DE for detecting MI with a sensitivity of 100% versus 90% (p=0.03) and accuracy of 100% versus 89% (p< 0.01). Specificity was also higher for FIDDLE, however did not reach statistical significance (100% v 87%; p=0.5). For subendocardial infarcts (≤25% transmural), the sensitivity of BN-DE dropped to 81% (p=0.03) and accuracy to 85% (p< 0.01). Figure 2 shows typical images in two patients with MI showing that contrast between blood pool and infarction is consistently high for FIDDLE but can be low for BN-DE. Not surprisingly, the MI-to-blood-pool CNR was higher for FIDDLE (57.8±37.6) compared to BN-DE (7.9±19.7; p< 0.0001). Figure 3 demonstrates that blood pool homogeneity can occasionally be poor for BN-DE. This is likely due to the short inversion time required for BN-DE imaging which may accentuate small differences in apparent T1 due to flow effects, B1 inhomogeneity, etc.
Conclusion: FIDDLE provides improved diagnostic performance compared to BN-DE particularly in subendocardial infarcts. Gray blood techniques such as BN-DE may not detect infarcts when the T1 of blood and infarct are similar.
Figure 1: Comparison of signal intensities between FIDDLE and BN-DE imaging in a control patient without MI. Cine imaging and conventional DE-CMR images (left) show region of analysis (orange line). Note BN-DE image has a suppressed blood pool signal compared to DE-CMR (e.g “gray-blood”). However, normal myocardium has lower image intensity (e.g. is black). For FIDDLE, the cavity signal is black whereas normal myocardium has higher image intensity (e.g is “gray”).
Figure 2: Comparison of signal intensities between FIDDLE and BN-DE in two patients with MI. A) MI has high conspicuity for both FIDDLE and BN-DE, although blood pool-to-infarct CNR is higher for FIDDLE. B) MI has divergent conspicuity between techniques, where FIDDLE easily detects the MI while in BN-DE the blood pool-to-infarct CNR is low since both blood pool and infarct are gray.
Figure 3: Blood pool inhomogeneity is seen in BN-DE images (center) which are absent for DE-CMR (left) and FIDDLE (right).
