Oral Case
MARIA BOUTSIKOU, MD, PhD, MSc, FESC, FSCMR
MRI/CT UNIT DIRECTOR
MEDITERRANEO HOSPITAL, Greece
MARIA BOUTSIKOU, MD, PhD, MSc, FESC, FSCMR
MRI/CT UNIT DIRECTOR
MEDITERRANEO HOSPITAL, Greece
GEORGE SEVASTOS, MD
CONSULTANT CARDIOLOGIST
MEDITERRANEO HOSPITAL, Greece
Dionysios Tsilidis
JUNIOR DOCTOR
MEDITERRANEO HOSPITAL, Greece
Evaggelos Vernardos
MRI/CT UNIT RADIOGRAPHER
MEDITERRANEO HOSPITAL, Greece
GEORGE KANOUPAKIS, MD
RADIOLOGIST
MEDITERRANEO HOSPITAL, Greece
A 49 year old male with no previous medical history, was admitted to the A&E due to pain at the right anterior chest wall radiating to the back the last 3 days. He had family history of coronary heart disease. The patient was a marathon runner and he had his last uneventful race one week before his admission.
Diagnostic Techniques and Their Most Important Findings:
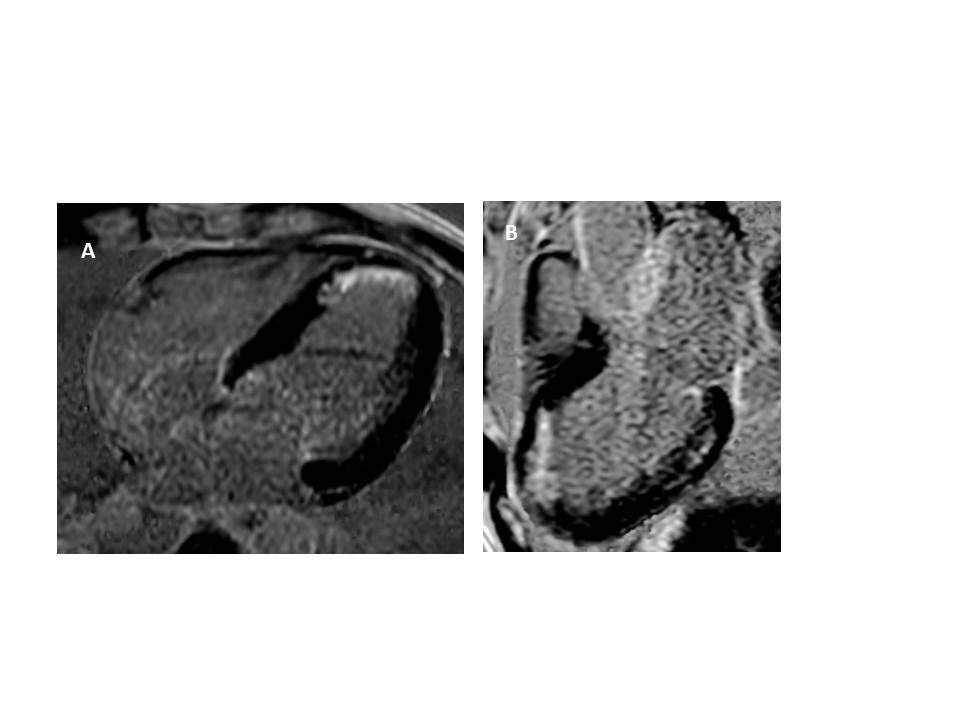
There were no abnormal findings on clinical examination. His blood tests showed a borderline increase in his troponin levels with normal CPK-MB levels. His ECG had no signs of ischemia. The patient was admitted for 48h monitoring and further testing. During his hospital stay he remained asymptomatic with no ECG changes or further increase of the cardiac biomarkers. After 48h he was discharged and referred for an exercise stress test which was negative for ischemia. The patient was referred for a cardiac MRI study to exclude any myocardial injury. Cardiac MRI study showed late myocardial enhancement at the subendocardial region of apical anterior septum as well as mid-wall enhancement at the basal posterior wall. A coronary angiogram was subsequently performed which showed a significant stenosis at the distal part of the left descending artery. PCI at the distal LDA followed
Learning Points from this Case:
Subclinical coronary artery disease has been previously shown to be present in high endurance athletes. Specifically in a recent study comparing master athletes with low cardiovascular risk with matched controls, athletes had predominately calcific plaques while training was and independent factor for higher calcium score or luminar stenosis. Endothelial damage from increased shear stress forces may be one of the mechanisms for increased plaque burden in master athletes. Late myocardial enhancement at the mid-wall of septum and posterior wall are common findings in high endurance athletes undergoing a cardiac MRI.
References
< ![if !supportLists] >1. < ![endif] >Merghani A et al. Prevalence of subclinical coronary artery disease in Masters Endurance athletes with a low atherosclerotic risk profile. Circulation 2017; 136: 126-137.
< ![if !supportLists] >2. < ![endif] >Aengevaeren V et al. Relationship between lifelong exercise volume and coronary atherosclerosis in athletes. Circulation 2017; 136: 138-148.
Figure 1. Cardiac MRI, LGE images: (A) four chamber view- subendocardial enhancement at the apical anterior septum (B) three chamber view- subendocardial enhancement at the apical anterior septum and mid-wall enhancement at the basal posterior wall.