
Quick Fire Cases
Andres M. Tavera-Paredes, MD
Cardiac imaging fellow
Instituto Nacional de Cardiología Ignacio Chávez, Mexico
Cayo Miguel Angel Leveau-Luján, MD, MSc
Fellow of Cardiac Magnetic Resonance and Angiotomography
National Institute of Cardiology "Ignacio Chávez", Mexico
Cayo Miguel Angel Leveau-Luján, MD, MSc
Fellow of Cardiac Magnetic Resonance and Angiotomography
National Institute of Cardiology "Ignacio Chávez", Mexico
Miguel Cruz, MD
Medical physician of cardiac magnetic resonance
National Institute of Cardiology "Ignacio Chávez", Mexico
Aloha Meave Gonzalez, MD
Chair
Instituto Cardiologia, Mexico
CMR was performed on a Philips Ingenia 3 Tesla scanner. Balanced steady state free precession cine sequences were acquired to profile the anatomy and assess ventricular parameters. A non-ECG gated dynamic MRA and an ECG and respiratory navigated 3D MRA (mDixon) were acquired using a slow-infusion protocol with a split-bolus of gadobutrol. Velocity-encoded 2-dimensional (2D) flow sequences and a non-contrast-enhanced 4D flow sequence were acquired. The CMR showed:
Given the patient’s asymptomatic status, normal LV mass, and function, the decision was made to follow the patient clinically and plan for an LVOT revision at the time of the next RV-PA conduit revision, or sooner as clinically indicated. CMR was extremely helpful for a comprehensive evaluation of this patient’s anatomy and physiology, and to inform the timing of surgical intervention. Though rare, late intracardiac obstruction can occur after VSD closure to an RV-origin aorta or neoaorta; CMR is diagnostic and provides additional anatomic and physiologic data to guide management.
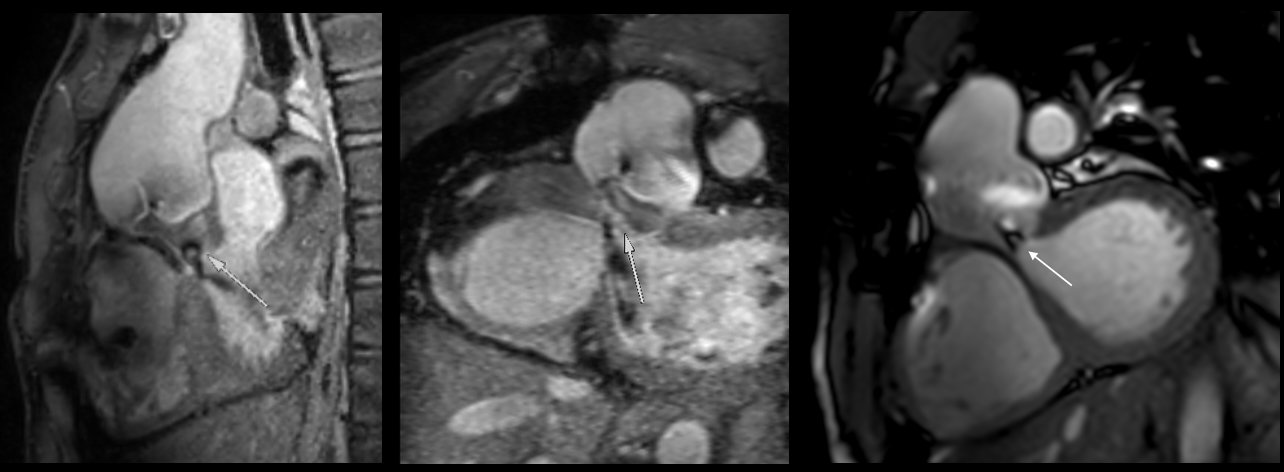
VSD restriction
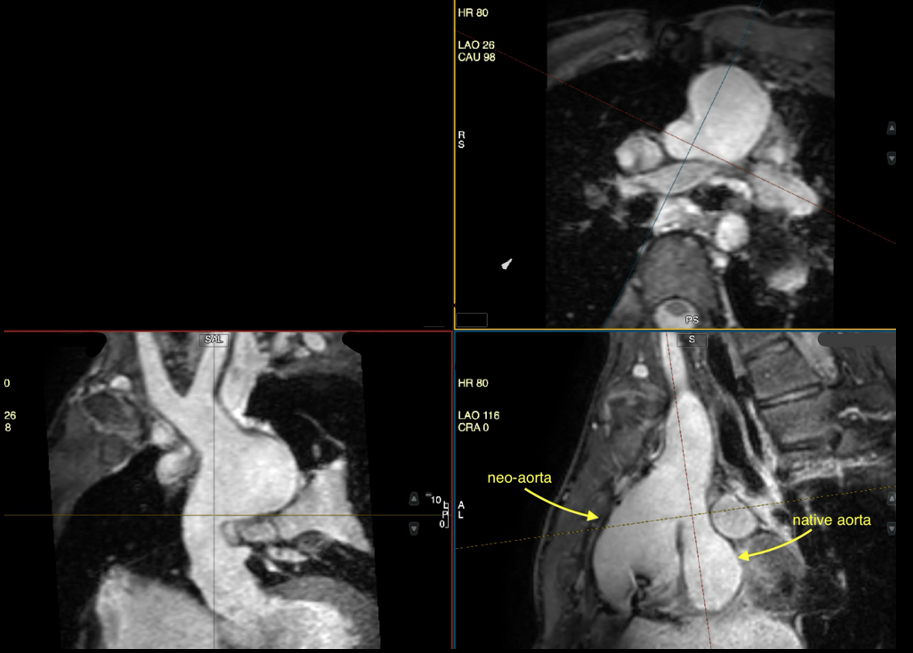
Native aorta, DKS and neo-aorta
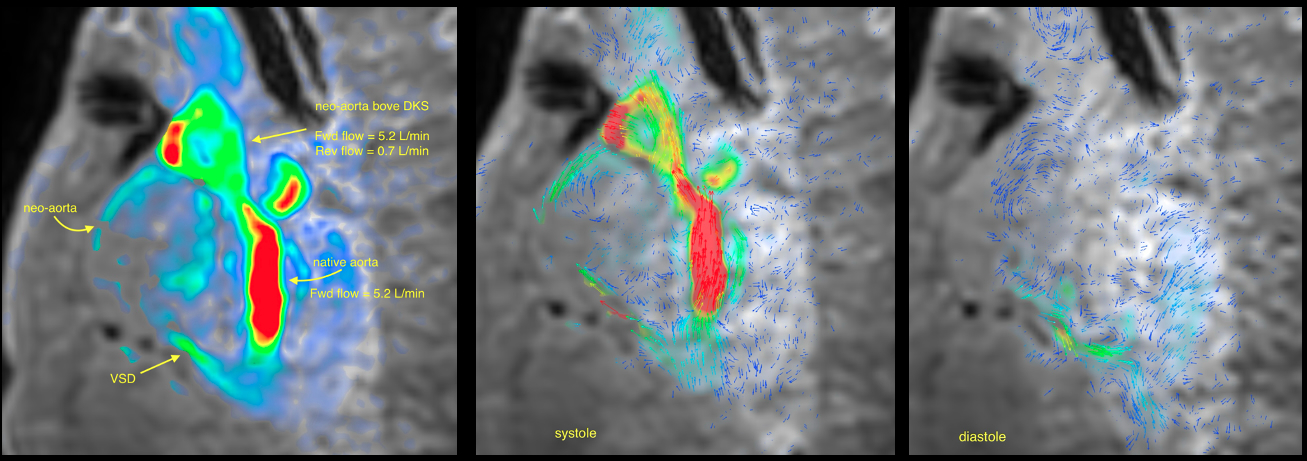
4D flow visualization of restrictive VSD and aortic flow
VSD restriction
Native aorta, DKS and neo-aorta
4D flow visualization of restrictive VSD and aortic flow
