Oral Case
Mansi Verma
Assistant Professor
IGMC Shimla, India
Mansi Verma
Assistant Professor
IGMC Shimla, India
Anupam Jhobta, MD
Professor
IGMC Shimla, India
Case 1: A 61-year-old male patient, hypertensive and chronic smoker presented with acute chest pain. He had previous two episodes of inferior wall ST elevation myocardial infarction (STEMI) in the past. Electrocardiogram (ECG) showed non-ST elevation in inferior leads. Echocardiography revealed left ventricular ejection fraction of 36% with mild mitral regurgitation. In addition, there was evidence of large cavity (40 x40 mm) adjacent to the mitral valve communicating with the left ventricle (LV). Coronary angiogram suggested plaques in left anterior descending artery (LAD) with 90% stenosis in left circumflex artery (LCx) and chronic total occlusion of right coronary artery (RCA).
Case 2: A 58-year-old male patient, smoker presented with chest pain. ECG revealed ST elevation in inferior leads. Echocardiography demonstrated regional wall motion abnormality (RWMA) in RCA territory with mild LV systolic dysfunction. On angiography, there was total occlusion of RCA with 70% stenosis in LCX. Percutaneous coronary intervention to RCA was performed and was uneventful. Echocardiography done after the procedure demonstrated outpouching from the basal inferior wall of LV with mild LV systolic dysfunction.
Case 3: A 53-year-old male presented with acute chest pain and palpitations. Echocardiography revealed wide complex tachycardia and external electric shock was given. He was diagnosed with acute coronary syndrome: non-STEMI in the current visit. Cardiac Troponin was raised (4.6 ng/mL). Echocardiography revealed RWMA in LCx territory with a focal outpouching from basal lateral wall of LV.
Diagnostic Techniques and Their Most Important Findings:
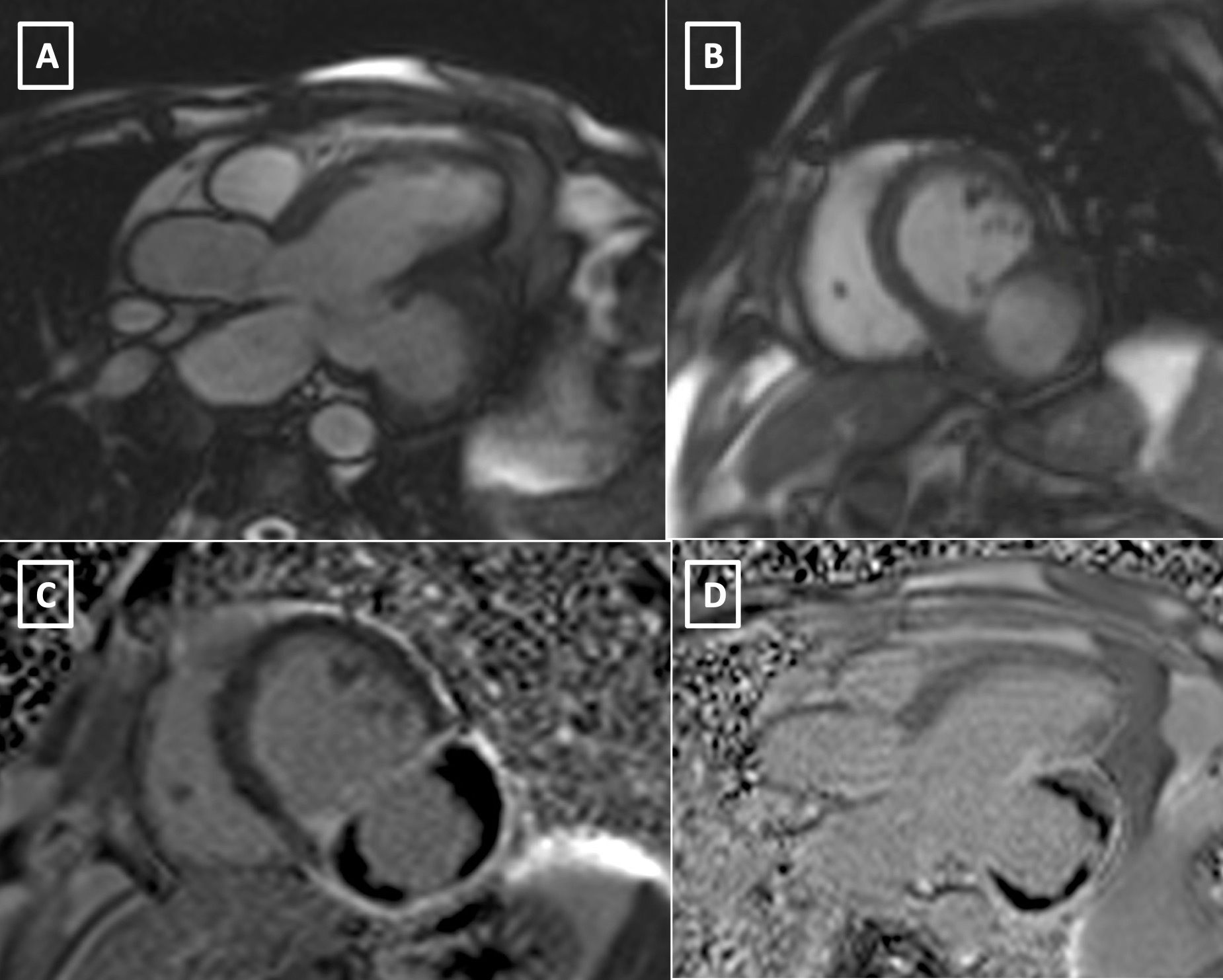
Case 1: Cardiac magnetic resonance imaging (CMR) done for further characterization of this cavity demonstrated wide necked large multiloculated outpouching from the inferior and inferolateral basal LV wall in submitral location. The largest contrast filled outpouching measured 32 x 30 mm. Late gadolinium enhanced image revealed non-enhancing thrombus and overlying thinned aneurysmal wall with transmural enhancement. (Figure 1) The patient was discharged on dual antiplatelets, statins and beta blockers and is on regular follow up.
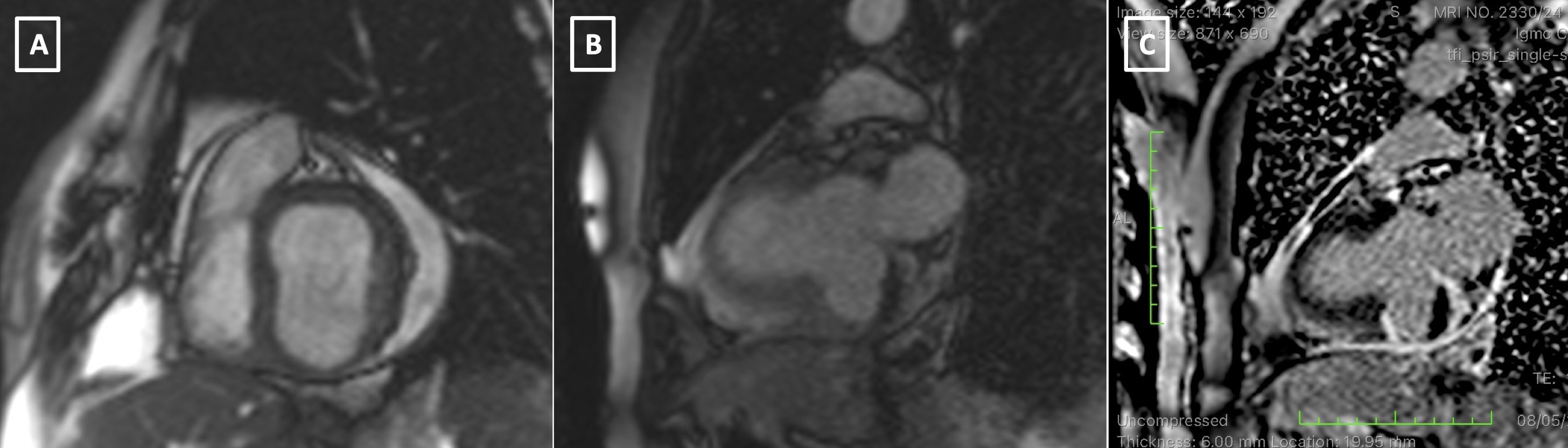
Case 2: CMR confirmed large aneurysm measuring from basal inferior segment near the mitral valve measuring 24x29 mm and pericardial effusion. (Figure 2) Considering the transmural late gadolinium enhancement of aneurysmal wall, myocardial infarction was the likely cause. He was prescribed dual-antiplatelets, statins and beta blockers and is doing well at follow up visit.
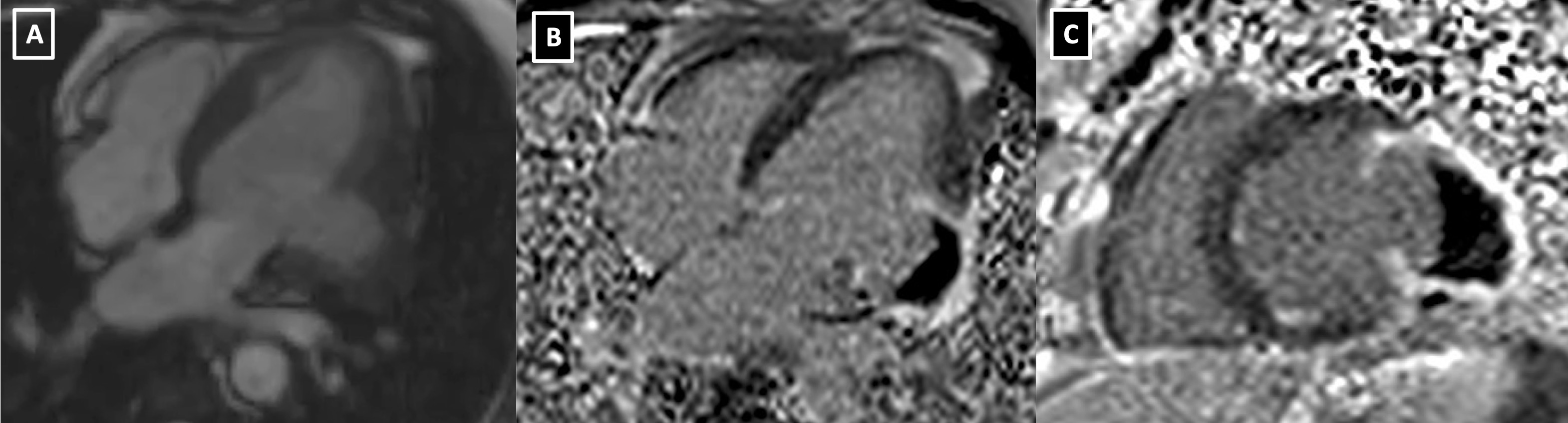
Case 3: CMR confirmed submitral aneurysm from basal lateral LV wall with transmural enhancement and large non-enhancing thrombus. (Figure 3)
Learning Points from this Case:
Submitral aneurysm is a rare cardiac pathology and most commonly occurs due to congenital defect in posterior portion of mitral annulus. We hereby reported three cases of submitral aneurysms with the cause being coronary ischemia. Coronary artery disease related aneurysms are usually apical. However, rarely can occur in submitral location as a consequence to myocardial infarction and we must be vigilant in such cases with atypical presentation. Multimodality imaging including cardiac magnetic resonance imaging helps in delineating underlying etiology and identifying the exact size, location, extent and relationship of the aneurysm. Our case series is unique in that it presents submitral aneurysm of ischemic aetiology and the causal relationship has been well established.