ISMRM - SCMR Workshop

Andrew D. Scott, PhD, FSCMR
Senior Lecturer
Imperial College London and Royal Brompton Hospital, United Kingdom
Andrew D. Scott, PhD, FSCMR
Senior Lecturer
Imperial College London and Royal Brompton Hospital, United Kingdom
.jpg "Pedro F. Ferreira, PhD photo")
Pedro F. Ferreira, PhD
CMR Physicist
Royal Brompton Hospital, United Kingdom
Ricardo Wage, RT, FSCMR
Chief CMR radiographer
Royal Brompton & Harefield NHS Foundation Trust, United Kingdom
Karl P. Kunze, PhD
Senior Cardiac MR Scientist
Siemens Healthineers, United Kingdom

Dudley Pennell, MD, PhD
Professor
Imperial College London, United Kingdom

Sonia Nielles-Vallespin, PhD, MSc, BSc
Senior Lecturer
Imperial College London
Recent work1,2 has demonstrated the ability of diffusion tensor CMR (DTCMR) to detect focal pathological changes in myocardial microstructure non-invasively and provide potential prognostic information. However, DTCMR protocols typically image only the mid myocardium or provide sparse ventricular coverage. Recently, commercially available ultrahigh strength gradient systems have become available in whole body systems, which can substantially shorten TE for motion compensated spin echo (MCSE) DTCMR and enable more efficient protocols.
In this work we demonstrate whole LV coverage in a DTCMR protocol making use of ultrahigh gradient strengths, reduced field of view excitation and interleaved slice imaging to deliver whole LV coverage in < 25minutes. We provide reference values in a cohort of healthy volunteers demonstrating systematic differences in microstructural parameters across the LV myocardium.
Methods:
A second order MCSE DTCMR research sequence with single-shot EPI readout was implemented on a 3T scanner with 200mT/m, 200T/m/s maximum gradient strength and slew rate respectively (MAGNETOM Cima.X, Siemens Healthcare AG, Erlangen Germany). Protocol parameters included, FOV=360x135x8mm3, acquired resolution 2.4x2.4mm2 (1.2mm2 reconstructed), 2D spatially selective excitation (ZoomIt) to reduce the phase field of view, fat sat, TE=58ms, TR=2RR intervals. One b=0 and 6 encoding directions at b=500smm-2 (8 averages) or b=50smm-2 (2 averages) were acquired per breath hold and 2 slices were interleaved within an 18 RR interval breath hold, triggered to mid-systolic contraction (TD=150ms). Slices covered LV base to apex with a 2mm inter-slice gap.
DTCMR processing was performed using an in-house Python tool (INDI - https://github.com/ImperialCollegeLondon/INDI) including frame rejection, non-rigid b-spline registration, segmentation, non-linear weighted least squares tensor fitting. DTCMR data was compared between levels (basal, mid and apical, defined based on equal division of the LV in the long axis) and between septal and free walls.
Results:
20 healthy volunteers were recruited (10 male; mean 36, range 20-51 years).
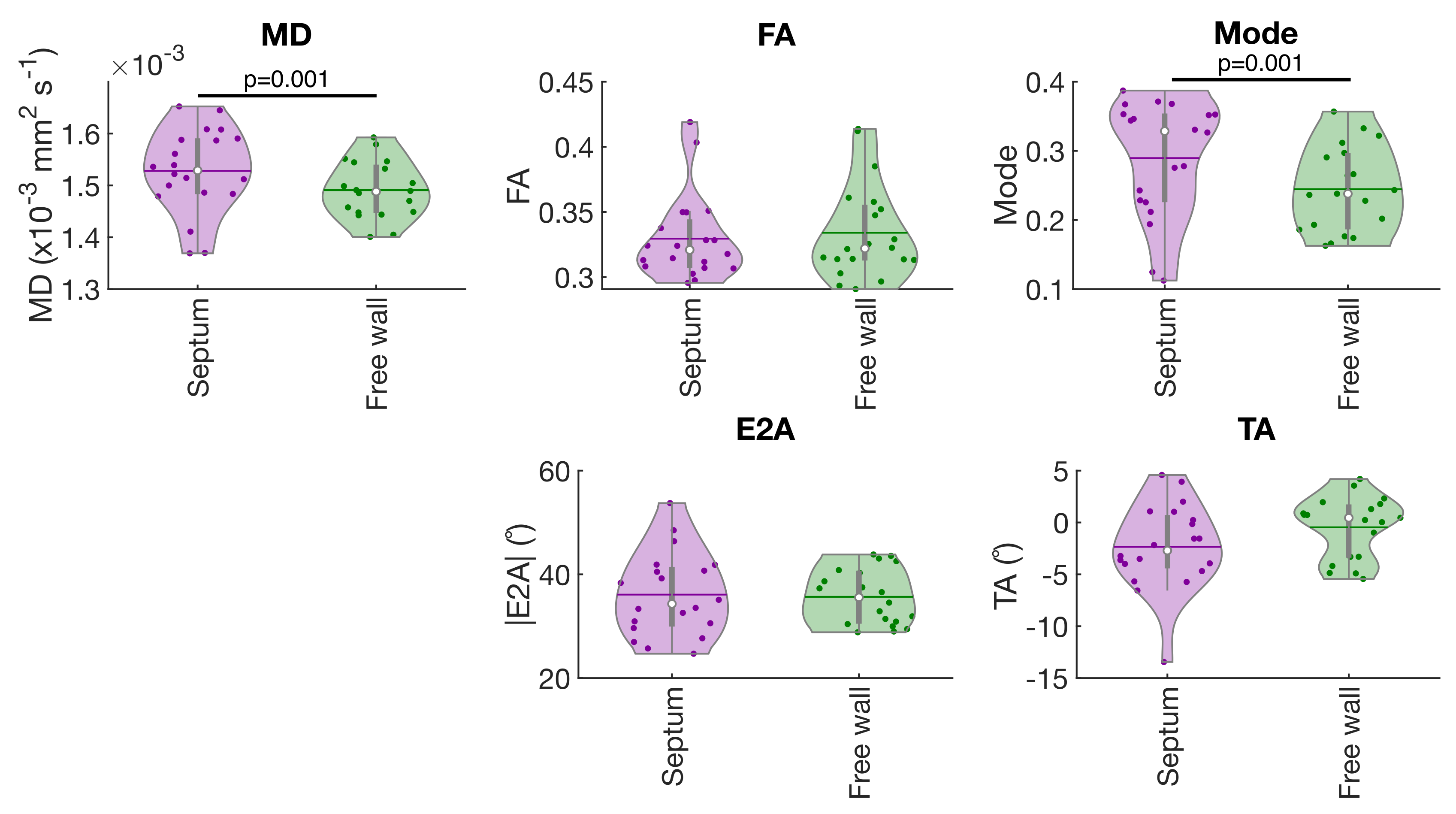
DTCMR data was acquired and processed from all subjects with an effective median [IQR] scan time of 24 [6] mins. Figure 1 shows example helix angle (HA), sheetlet angle (|E2A|), fractional anisotropy (FA) and mean diffusivity maps (MD), demonstrating high quality data from basal to apical slices. Figure 2 compares DT-CMR parameters between levels, highlighting: significant reductions in the magnitude of transmural HA gradient in the base perhaps as a consequence of reduced basal SNR; reductions in apical |E2A| and changes in transverse angle (TA) between levels, perhaps reflecting the more complex apical microstructure. In contrast, MD was significantly increased in the septum relative to the free wall, but |E2A| and TA were not different between walls (figure 3).
Conclusion:
We present a DTCMR protocol delivering coverage similar to that achieved with more traditional techniques such as LGE, requiring < 25minutes. We show initial normal values for reference and measure regional differences in microstructure across the myocardium. Future work will evaluate this efficient DT-CMR technique in clinical cohorts.
Figure 1: Example DT-CMR maps obtained in one healthy subject covering the LV myocardium from the basal to apical regions.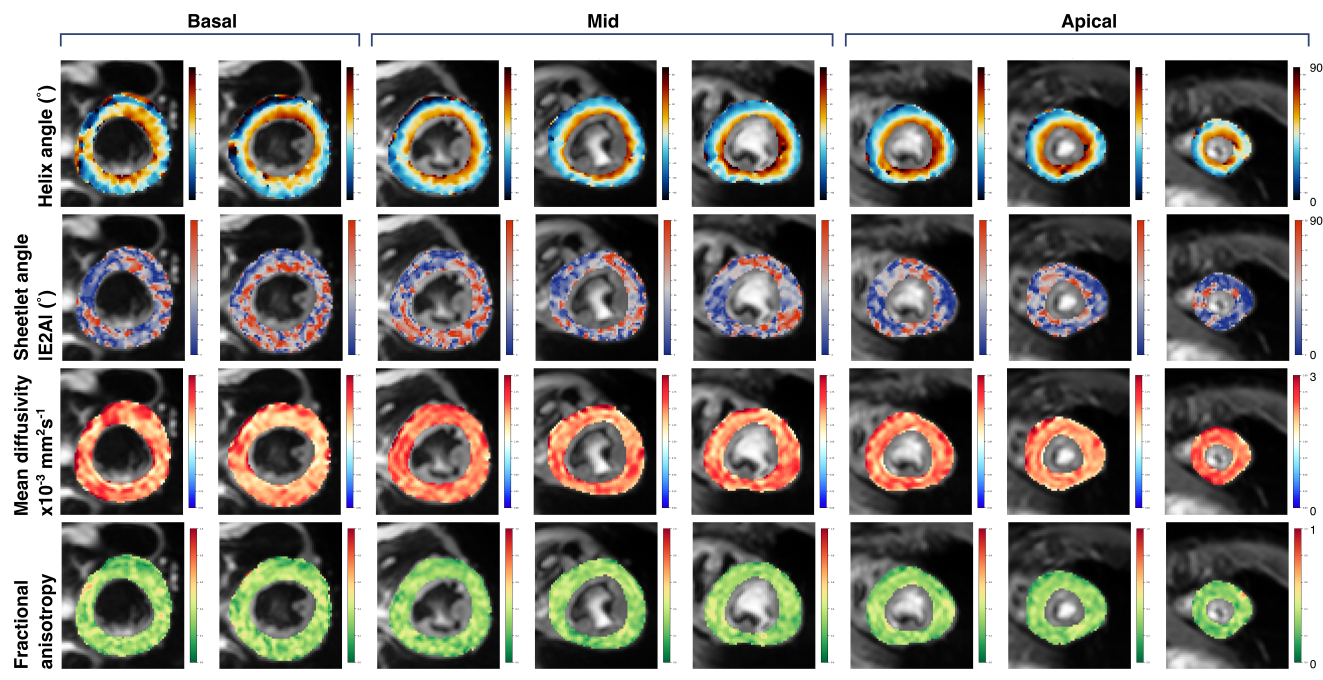
Figure 2: A comparison of DT-CMR parameters between mid and basal slices; and mid and apical slices in the 20 healthy volunteers. P-values are shown where comparisons show significant differences between levels (p < 0.05 significant).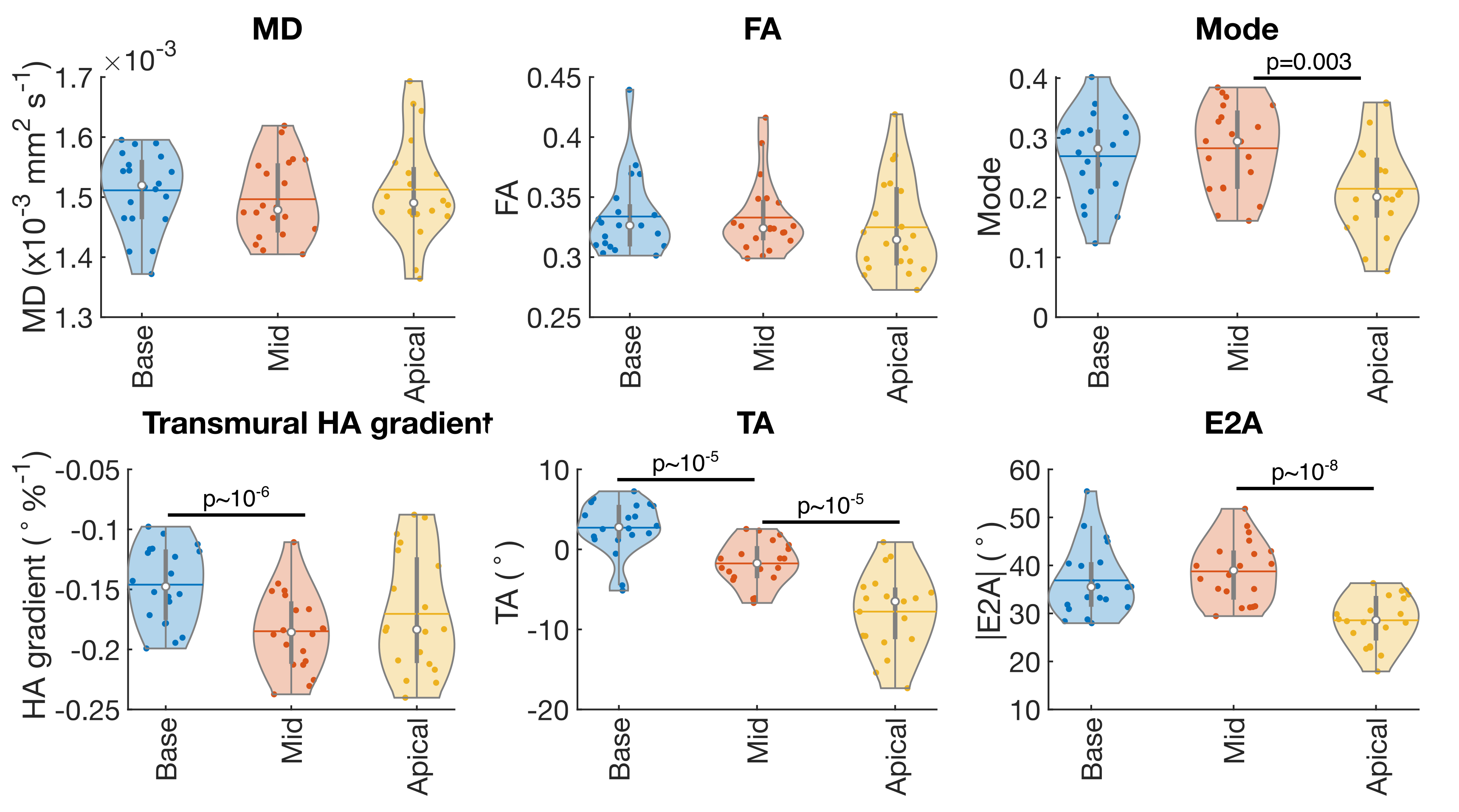
Figure 3: A comparison of DT-CMR parameters between the septal and free wall. P-values are shown where comparisons show significant differences between levels (p < 0.05 significant). Current analysis methods do not provide transmural HA gradient by segment.